Introduction
Population health indicators are significant characteristics of the residents of a geographic area used as supporting evidence to understand that population’s physical or mental state. These indicators are primarily used to measure a population’s health risk.1 Often, it is useful to compare the health of populations from different geographic areas.1,2 For this, a population health index (PHI) may be used because it combines a set of indicators into a single indicator that is normalized, standardized, and scaled.3 Researchers and policymakers assess and compare the health of areas with PHIs by determining the impact of health policy interventions across locations, assessing inequalities, and monitoring health trends over time.2,4
Ashraf et al. (2019) performed a scoping review and found articles describing 27 PHIs.2 Their review updated Kaltenthaler et al.'s (2004) review on the same topic.5 While the earlier review5 focused more on the methods of developing and potentially combining PHIs, the more recent review2 emphasized that only a few PHIs measure specific health topics or subpopulations. Furthermore, there is a gap in the literature about how general PHIs are used for researching particular diseases. To better determine the usefulness of PHIs in measuring the outcomes of a specific disease, this review focuses on the use of PHIs in cancer research. Cancer is the second leading cause of death and is trending to become the top cause worldwide,6 contributing to nearly 20 million deaths in 2020.7
While several PHIs can be used, the most common is disability-adjusted life years (DALYs).8 DALYs are “the sum of the present value of future years of a lifetime lost through premature mortality, and the present value of years of future lifetime adjusted for the average severity (frequency and intensity) of any mental or physical disability caused by a disease or injury”.9 In the DALYs approach, on a scaling pattern, each state of health is assigned a disability weighing from perfect health (zero) to death (one).10 Two organizations, the World Bank and the World Health Organization, launched DALYs11 and have been using them for over two decades to quantify the burden of diseases and help determine cost-effectiveness in the economic evaluation of health interventions and programs.12
In this scoping review, our goal was to determine for what purposes cancer-related research articles use PHIs, in what countries this research has taken place, and for what types of cancer sites (e.g., breast, colon). The findings of this review will inform cancer researchers who may consider using PHIs in their research so they can better know how these measures can be helpful. It will also help policymakers better understand the relevance of funding population health data collection, as such data is the cornerstone of population health index values and a major determinant of index accuracy.
Materials and methods
Search Strategy
We used the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines13 and conducted database searches (through September 2021) in PubMed (including MEDLINE), CINAHL, and Web of Science. The keyword strings used to capture relevant studies were “cancer” and the name of 25 of the 27 indices from the2 article. We also searched for two additional terms along with “cancer”: “health-adjusted life years” and “population health index” because they were not included in the list from the article.2 The two indices we did not include from the Ashraf et al. article were: 1) Quality-Adjusted Life Years because it is the academic standard for drug and medical treatment cost-effectiveness research and would have made this review impossible due to the high volume of articles, and 2) Index of Multiple Deprivation because it is a socio-economic measure rather than a population health measure. Any article with our keyword strings in either the title or the abstract was included in the initial review.
Study Criteria
We eliminated all duplicate studies, and then two researchers independently screened each abstract using the following inclusion criteria: the study was related to cancer and used a PHI. We included all types of study designs, countries, sample sizes, and article languages. Since PHIs are relatively new, we did not have a beginning date constraint. After screening abstracts, two researchers retrieved and reviewed full-text articles independently for inclusion. The researcher team discussed and resolved any discrepancies.
Data Extraction
For each study meeting the inclusion criteria, two researchers independently extracted key information, including the study design, cancer site, study aim, findings, and whether vulnerable and key populations were included. In determining vulnerable and key populations, we used the United Nation’s definition: “populations that live in poverty without access to safe housing, water, sanitation and nutrition and those who are stigmatized, discriminated against, marginalized by society and even criminalized in law, policy and practice”.14
We determined each study’s quality based on the Quality Assessment Tool for Quantitative Studies.15 This tool assesses various factors of a study and results in a “strong,” “moderate,” or “weak” rating. Note that while we did not exclude qualitative studies, all the studies found were quantitative. As with the article inclusion process, any discrepancies in extraction results were discussed and resolved among the researchers.
Results
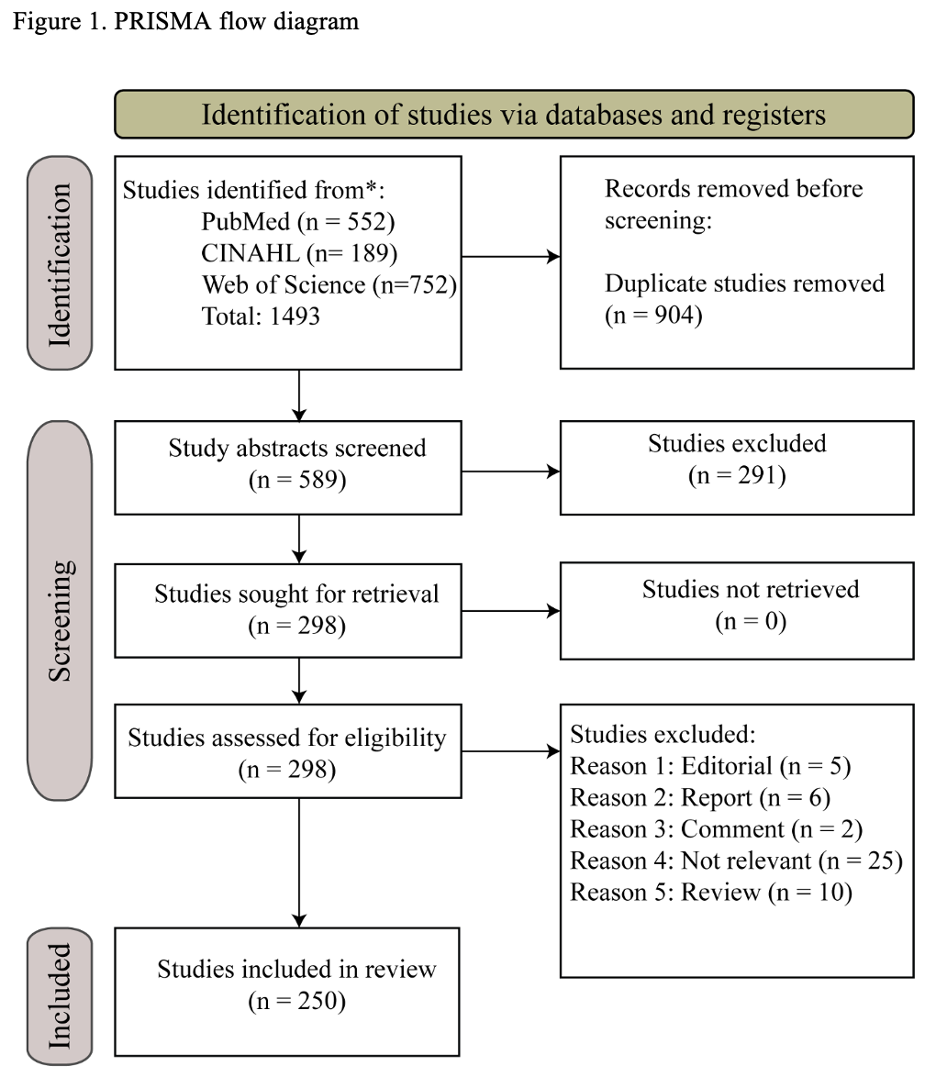
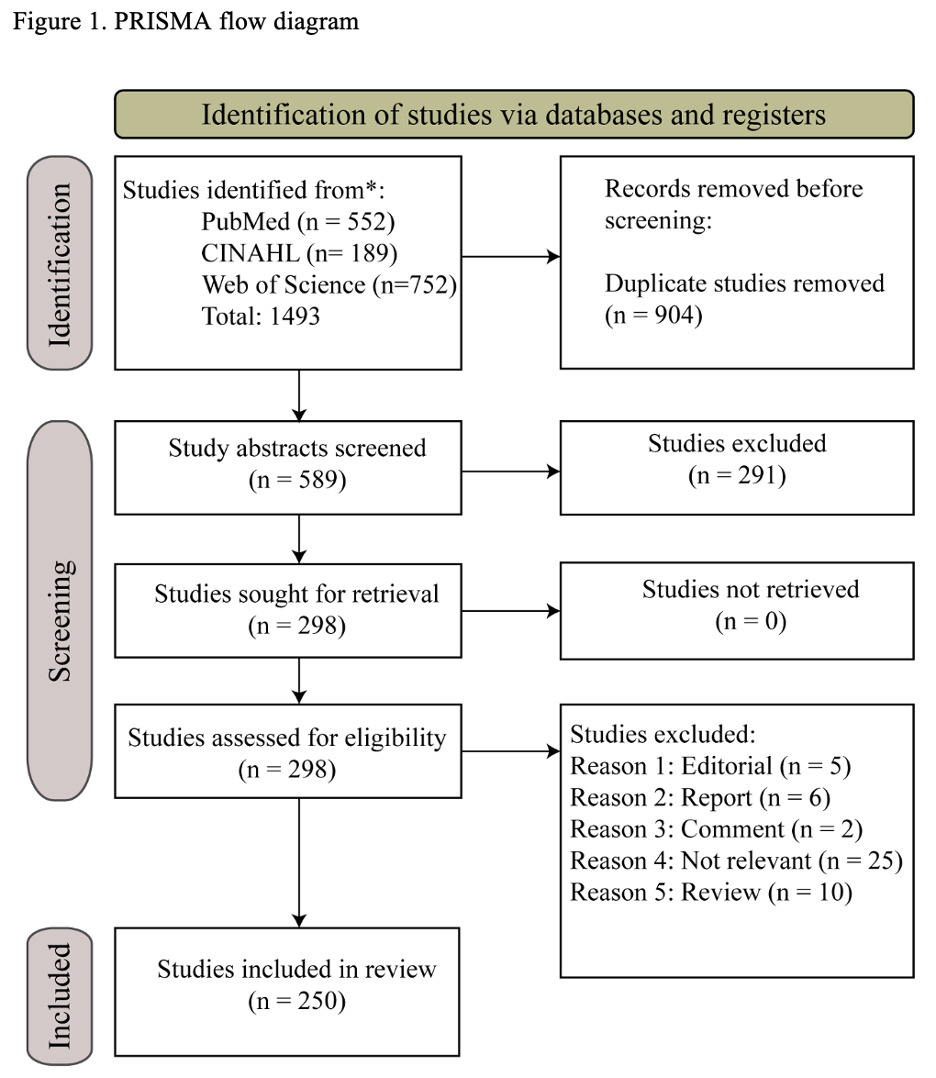
A total of 1493 articles were initially retrieved from PubMed (552), CINAHL (189), and Web of Science (752). After removing duplicates and screening abstracts, we reviewed 298 peer-reviewed articles in full. Of these articles, 48 were excluded for the following reasons based on the following criteria: editorial (n = 5), report (n = 6), comment (n = 2), not relevant (n = 25), or review (n=10). The remaining 250 articles were included in our analysis. Figure 1 highlights the selection process suggested by PRISMA guidelines.13
Article types
Table 1 shows the frequency distributions of countries of the reviewed studies. Most studies focused on the entire world (n=77), followed by China (N=48). Fifty-one specific countries were represented in the articles. High-income or upper-middle-income countries were represented 149 times, lower-middle-income countries 32 times, and low-income countries four times. Table 2 shows the frequency distributions of cancer sites included in the articles. The greatest number of studies focused on general cancer sites, defined for purposes of review as representing more than five cancer sites (n=70), followed by breast cancer (n=39), cervical cancer (28), lung cancer (26), colon cancer (18), and liver cancer (18).
Data quality
In terms of article quality, we found a mix of high-quality (n=86), intermediate-quality (n=131), and low-quality (n=33) articles. For all articles, we examined the journal’s impact factor. The average impact factor of the journal for the articles was 6.50. The average difference between the data collection date and the article publication date was almost 11 years. A Supplementary Appendix can be found online with a summary of all the studies.
Study aims
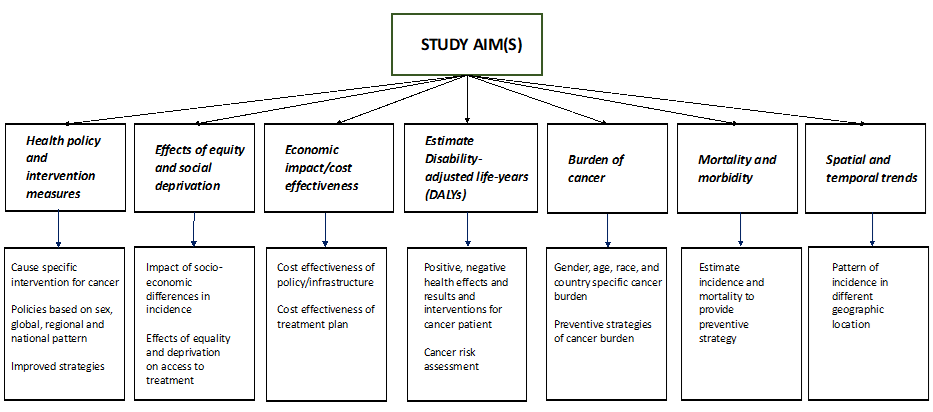
Figure 2 shows the classification and sub-classification of the primary aim(s) of studies using PHIs in cancer research. Such studies sometimes examine what level of burden cancer is for various demographic groups. Additionally, specific mortality and morbidity outcomes are often the focus. Cancer studies using PHIs examine policies, interventions, economic impact, and spatial and temporal trends.
.png)
Discussion
Our review reveals that PHIs are used in cancer research for various aims. The purposes of these studies range from measuring outcomes to determining more effective policies and interventions. PHIs also allow for spatial and temporal comparisons in cancer research. Additionally, some researchers use PHIs to determine economic outcomes and the cost-effectiveness of programs and policies. While many cancer studies using PHIs involve DALY, other PHIs have also been used.
There are 149 instances of high-income and upper-middle-income countries represented in the studies. Conversely, just 36 instances of low-income or lower-middle-income countries appear. This finding is consistent with other research showing that cancer research is heavily skewed toward higher-income countries.17 Low- and middle-income countries face a rapid increase in noncommunicable diseases, including cancer.17 Therefore, researchers must research in low- and middle-income countries to help inform policies and programs to help prevent and control cancer.
The most common types of cancer worldwide are lung, breast, colon, and prostate cancers, accounting for more than 40% of cancer diagnoses.18 Many studies in our study focused on lung, breast, and colon cancer. However, relatively few focused on prostate cancer. One explanation may be that many studies related to prostate cancer do not have as convincing rejections of the null hypothesis as for other cancers. Often, research that fails to reject the null hypothesis does not get published.19
The quality of the cancer studies that used PHIs varies, as indicated by the article quality ratings in our review. However, most studies were of strong or moderate quality. Furthermore, the high average journal impact factor for the articles in our review indicates that PHIs may be useful measures in impactful cancer research.
An element that stood out in this review is that the data is sometimes too old or incomplete. This is of particular concern for low- and middle-income countries where cancer registration data and quality indicators can be incomplete or unreliable.1 Diagnostic and treatment capacity limitations often cause underestimations of cancer incidence.20 Poor data quality indicates a lack of collaboration among reporting sources and the inability of the registrar to perform quality abstracting.21,22 Periodical discontinuity of registration, extrapolation of regional data to the national level, and under-reporting of cancer are other recognized common sources of bias in cancer-related data.23 Harrison et al. (2020) presented similar limitations regarding data quality in low- and middle-income countries regarding immunization programs.22
The lack of accurate cancer registry data is of particular concern for low- and middle-income countries. Just 20% of countries have sufficient quality cancer data to determine incidence rates.24,25 Furthermore, data about cancer sites and stages are not collected or not well defined in many low- and middle-income countries.24,26,27 An initiative established in 2011 by the International Agency for Research on Cancer (IARC) in partnership with other international organizations to improve cancer registries globally is the Global Initiative for Cancer Registry Development (GICR). The GICR has six regional hubs to work with countries to support registries and provide training and research opportunities.28 More efforts like this are necessary to improve cancer data collection and research across the globe.
This scoping review is subject to a few limitations. First, this review was limited to peer-reviewed studies. It is possible that there were cancer studies using PHIs that were not published as peer-reviewed articles and, therefore, were omitted here. Second, there was heterogeneity in the research methods across studies. Thus, we did not perform a quantitative meta-analysis to examine PHI use in cancer research. Lastly, not all the studies reviewed were of high quality. We chose to include all the articles ranging from high to low quality for a comprehensive view of the literature in this space. However, the lower-quality articles influenced the study aims summary and frequencies the same way the higher-quality articles did. That is, we did not put more weight or emphasis on those articles we deemed as higher-quality.
Our review highlights areas for potential improvement in using population indices in cancer research. First, there were 27 cancer sites with five or fewer studies incorporating population indices. Two-thirds of the cancer sites had just two or fewer studies, including population indices. With five cancer sites having 18 or more studies each that used such indices, our review indicates an opportunity to use population indices to help measure cancer occurring in more sites. Second, cancer researchers may consider using population indices other than DALY for their studies. Interestingly, fewer studies were of low quality for the studies using non-DALY indices than the DALY indices (10.5% vs 13.4%). While DALY may work best for many studies, our review may help raise awareness about other population indices that could be helpful in cancer research.
This scoping review examined the body of literature to date that used PHIs to study cancer. There are several aims that such studies use PHIs to investigate cancer. This review shows that PHIs can be useful in studying cancer topics. However, caution must be observed in using outdated or missing data in studies relying on PHIs. Furthermore, future research should investigate the use of PHIs in low-income and lower-middle-income countries to develop a better understanding of which to base cancer prevention and control decisions. Finally, when developing new PHIs, it may be helpful to illustrate the PHI’s use for studying particular diseases so that more disease-specific researchers can use these population measurement tools.
Ethics approval
No ethics approval was required for this scoping review of published data.
Funding
Funding to support the graduate research assistants came from the Illinois Innovation Network.
Authorship contributions
SA - Article selection, Data abstraction and curation, Formal analysis, Drafting the original manuscript, Reviewing and editing the manuscript. MV – Discussing article selection, Reviewing and editing manuscript. MCH – Conceptualization, Data abstraction and curation, Formal analysis, Drafting the original manuscript, Reviewing and editing manuscript.
Acknowledgments
The authors would like to thank Monica Kowalczyk for her help in retrieving and screeing articles. They would also like to thank Margaret Wright for sharing her expertise in cancer research to guide some discussion components.
Competing interests
The authors completed the ICMJE Unified Competing Interest form (available upon request from the corresponding author) and declare no conflicts of interest.
Additional material
Online Supplementary Document
Correspondence
M. Courtney Hughes, School of Health Studies, Northern Illinois University, US; courtneyhughes@niu.edu