Introduction
Sub-Saharan Africa (SSA) is the home to over 90% of all children (<15 years old) living with the Human immunodeficiency virus (HIV).1,2 Timely diagnosis of HIV infection is key to accessing antiretroviral therapy and reducing mortality and long-term morbidity.3–6 The World Health Organisation (WHO) recommends that HIV-exposed infants have a virological test at 4-6 weeks of age,3–5 yet worldwide, only 59% of children living with HIV have been tested compared to 82% of adults.3,5 In Malawi, only 51% of HIV-exposed infants received a virological test within the first 6 weeks of life, and only 52% of children (0-14 years) living with HIV were initiated on ART in 2017.7,8
Because of the persistence of maternal antibodies, nucleic acid tests which detect both Ribonucleic acid (RNA) and Deoxyribonucleic acid (DNA) are used for Early HIV infant diagnosis (EID), of which Polymerase chain reaction (PCR) is the gold standard.5,9–13 Although PCR is highly sensitive and specific, the reagents and equipment are expensive, and the assays must be performed by highly qualified staff. With only ten laboratories conducting PCR in Malawi, the samples must be transported some distance, leading to the risk of specimen loss and resulting in long turnaround times. For example, in 2017, the Malawi HIV unit reported an 8% loss of samples sent for HIV DNA PCR testing and time to HIV diagnosis by PCR took 2 to 3 months.7,8 This is substantially longer than the WHO recommendation of 30 days, contributing to a 33% loss to follow-up of HIV-exposed infants by 24 months of age.7,8 A possible solution to this problem would be the introduction of a fast, sensitive, specific, cost-effective HIV point of care test (POCT) that can be carried out in infants and children up to 18 months in district hospitals and local health care centres is desperately needed for early initiation of ART.
WHO and UNAIDS recommend that countries pilot and explore optimal ways of scaling up HIV testing.3,14 In Malawi, two WHO pre-qualified Point-of-care testing (POCTs), Alere q HIV1/2 Detect,14,15 and Cepheid Xpert HIV-1 Qual assay (XpertHIV),15,16 were piloted by Clinton Health Access Initiative (CHAI) in 2017 and have been used exclusively for research.14–16 The parent study on feasibility, acceptability and performance of XpertHIV confirmed that in comparison to PCR by Abbott, XpertHIV’s sensitivity and specificity were 100% (95% CI: 78.2 - 100%) and 100% (95% CI: 99.4 - 100%), respectively.17–20 The positive predictive value (PPV) and negative predictive value were 100% (95% CI: 78.2 - 100%) and 100% (95% CI: 99.4 - 100%), respectively.17,18 The positive and negative agreement between XpertHIV and PCR by Abbott were 100%, respectively. Despite the Cepheid GeneXpert machines being available in 114 health facilities throughout Malawi for TB diagnosis, in 2018, these machines were only used for TB diagnosis.21,22 The acceptability, feasibility, and usability of these POCTs depend on various factors such as the number of tests that can be processed simultaneously, availability of trained staff and requirements for sustained power supply. Real-world evaluation is therefore necessary and, given the existing resource constraints, in Malawi, assessment of cost and cost-effectiveness of XpertHIV is also needed.
The study aimed to provide costings evidence that policymakers could use for decision-making at a national level. We compared the costs of XpertHIV whole blood protocol (WB) against the standard of care HIV DNA PCR using Abbott systems (PCR). Our outcomes were cost-minimisation and cost-effectiveness using turn-around time (TAT) from sample collection to results.
Methods
Study setting and design
The study took place in Mulanje District Hospital, located in the Southern region of Malawi. Mulanje is a mountainous and tea-farming district on a border with Mozambique. The district is predominantly occupied by the Lomwe tribe and has an estimated total population of 428,322 and an adult HIV prevalence of 20.6%.23,24 Mulanje District Hospital is the secondary referral government hospital for 17 peripheral health centres in Mulanje district where ART is provided.
As a standard procedure for HIV-exposed infants in Mulanje and nationally, HIV tests were performed at six weeks, 12 months and 24 months as there is a chance that those born HIV negative can be infected through breastfeeding.7,8 Follow-up of HIV-exposed infants stops at 24 months of age or 3 months after cessation of breast feeding.7,8 EID testing for infants aged six weeks only involved DBS being sent to a molecular laboratory for PCR by Abbot testing and HIV 1 and 2 antibody tests for 12 and 24 months old, respectively.7,8
The standard of care and comparator (HIV DNA PCR by Abbott)
HIV DNA PCR using the Abbott M2000 machine was the comparator for this analysis and used to represent the existing EID strategy used in Malawi.7,8 For this study, DBS were prepared for HIV PCR testing at a central Queen Elizabeth Central Hospital (QECH) facility.
The intervention (Cepheid Xpert HIV-1 qual assay) XpertHIV))
XpertHIV detects HIV-1 total nucleic acid qualitatively from individuals suspected of HIV-1 infection using real-time PCR. It uses the GeneXpert Instrument (Cepheid, Sunnyvale, CA, USA), a closed, self-contained, fully integrated automated platform representing a paradigm shift in the automation of molecular analysis, producing results rapidly with minimal risk of contamination.16 The assay requires three steps: transfer 100 μl of whole blood into the cartridge’s large hole, dispense 750 ul elution reagent into the small hole in the cartridge’s insertion into the cartridge Xpert platform and start the run of the assay.16 For this study, all POCT XpertHIV testing was done on-site.
This costing study was nested within a prospective mixed-methods study that evaluated the feasibility, sensitivity, specificity, acceptability and usability of XpertHIV compared to HIV DNA PCR by Abbott systems using dried blood spots (DBS). The details of the setting and design of the parent study and HIV testing protocols are presented elsewhere.17–20
In brief, from July to August 2018, 680 children were tested,17,18 of whom 200 caregivers of children aged 0-14 who provided consent for HIV testing and costing study participants were recruited in Mulanje District Hospital (MDH) in southern Malawi. The current study compared costs of locally performed (XpertHIV) with DBS sent to QECH in Blantyre, 89 kilometres away, for testing by study PCR.
The study addressed testing for two groups- infants aged six weeks old only who were tested with XpertHIV, in-house PCR by Abbott at QECH and DBS sent to Thyolo District Hospital (TDH) for testing by PCR and the rest of the infants and children who had XpertHIV, in house PCR by Abbott at QECH and if over 12 months - HIV 1and 2 antibody tests.
Cost comparison Cepheid Xpert HIV-1 Qual assay (Xpert HIV) and HIV DNA PCR by Abbott systems (PCR)
We estimated health facility costs and economic costs borne by carers. Intervention-specific variable costs were estimated using the ingredients approach, while shared overhead costs such as waste management and utilities were apportioned by using the annual expenditure for a hospital. The latter were allocated to the laboratory using an allocation basis (estimated proportion of lab to hospital area), multiplying that by a proportion of the cost attributable to the study (e.g. proportion of lab electricity that a machine used for testing used) and multiplying that by the proportion of the study period to the financial year (29/365).
Fixed costs were annuitised using the standard formula,
K=E1−(1+r)−nr
where is the initial capital outlay, is the annual sum which at an interest rate for years will be equal to the initial capital outlay.25 Useful lives, of capital items were collected from different sources, and an interest rate of 3% was used.25 Capital items included the equipment and staff training.
Household costs included costs incurred by patients and guardians in seeking care, i.e. transportation, food, purchase of health passport, consultation, registration, laboratory test, medicines, gifts to health workers and under-the-table payments. This costing study randomly selected and recruited one out of every three caregivers from the parent study. The study estimated the opportunity cost of time that guardians and their companions spent travelling to health facilities and waiting for their child to get care, outpatient or inpatient. 2013 earnings data for the occupations represented in the household cost survey were adjusted for inflation using annual consumer prices indices for 2013 and 2018, multiplied by the times that each occupation category spent and converted into US dollars using a 2018 exchange rate of 1$ = MK750. Based on the simple random sampling, weights were applied to the costs, and an average patient cost was calculated. The weights were calculated by dividing the total number of clients observed during the study period by the costing sample size.
Cost-effectiveness analysis
We adopted a payer perspective, where the payer was the Government of Malawi. The cost per test was then estimated by dividing the total cost of each testing strategy by the sample size of n= 700. The standard formula for the incremental cost-effectiveness ratio (ICER) was used, with the difference in costs for the two strategies divided by the difference in their turn-around times.25 Turn-around time was calculated as a difference between when a sample was taken from a patient and when the test results were reported to the patient, expressed in days.
We conducted deterministic sensitivity analysis by extending the study period from 29 days to a year (365 days). We also conducted probabilistic sensitivity analysis by making 1000 Monte Carlo simulations and calculating the probability that a strategy could be effective at different threshold ratios. For each simulation, random draws were made from the Gamma distribution for cost data parameterised as in Microsoft Excel where and and the normal distribution for turn-around times.26 Cost data were categorised as equipment, human resources, lab consumables, overheads and transport for each strategy. Microsoft Excel was used when a draw was taken for each of these categories for each strategy.
Data sources
We used the Government of Malawi Integrated Financial Management Information System (IFMIS) expenditure data for the 2018/19 financial year for the Mulanje district health office and Queen Elizabeth Central Hospital to approximate overhead costs.27 Unit cost data were provided by the Principal Investigator, while data on waste management contracts were obtained from the Ministry of Health. Data on the useful lives of various equipment were obtained online and from other published literature.28 Data on household costs incurred in seeking care were collected through a costing survey questionnaire between July and September 2018. TAT data were compiled by laboratory staff at both centres as part of the study. Consumer price index data was obtained from the Reserve Bank of Malawi website.29 Open Data Kit was used to collect and manage data, and Stata-14 (StataCorp, Texas, USA) was used for analysis.
The College of Medicine Research and Ethics Committee (COMREC) approved the study protocol, informed consent forms, and questionnaires. (P.03/18/2378) and University College London Research Ethics Committee (13313/001). Written informed consent was obtained from the parent/guardian of each participant under 18. Children aged 0 to 14 years whose caregivers consented to HIV testing were enrolled in this study.
Results
From July to Sept 2018, 700 PCR by Abbott tests using DBS were performed on the 680 participants enrolled into the study, of whom 15 were identified to have HIV-positive results. These newly identified HIV-positive DBS were retested twice, and 5 of the 15 were retested three times, so with confirmatory testing of the HIV-positive cases, a total of 700 tests were performed. Costs of repeat tests were included in the analysis.
There were 49/680 blood samples insufficient for both PCR by Abbott and XpertHIV testing, so only PCR was done as it was the gold standard test. In total, 631 XpertHIV and 700 PCR tests were performed in the study.
Cost analysis
Table 1 shows the total costs incurred by each testing strategy broken down by major cost categories. XpertHIV was cost minimising compared to PCR Abbott for the same number of samples tested. XpertHIV had a total cost of $29,638.46 compared to $46,658.91 for Abbott PCR for the same number of samples tested. The average total cost of the XpertHIV test was $42.34 compared to $66.66 for PCR by Abbott.
The key cost drivers of the two strategies in Table 1 are equipment and lab consumables. PCR by Abbott has higher annuitised equipment costs representing 77% of the total cost compared to XpertHIV at 25%. However, XpertHIV has a higher cost for lab consumables representing 58% of the total cost and three times the cost of the corresponding items for PCR by Abbott.
Table 2 shows that the variable to fixed cost ratio for XpertHIV is 2.96:1 while for PCR by Abbott it is 0.30:1. This suggests that with a greater volume of tests, the average total cost of PCR by Abbott is likely to decline at a faster rate than XpertHIV or possibly be cost minimising compared to XpertHIV.
We tested this assumption by extrapolating the data from 29 days to a year (under the assumption of 240 working days.) We also considered the maximum capacity of the equipment for a year (11,856 tests for XpertHIV and 4608 for PCR by Abbott). The results are presented in Tables 3 and 4. Table 3 shows that the total cost of XpertHIV exceeds that of Abbott PCR, $191,147.88 and $124,700.21, respectively, reversing the base case scenario. However, the average total cost (ATC) per test is still lower for XpertHIV than PCR by Abbott, $16.12 and $27.06, respectively. The lower XpertHIV ATC is due to its higher capacity of tests in a year compared to PCR by Abbott. Based on Table 4, the variable cost to fixed cost ratio escalates to 23.3:1 for XpertHIV while it increases to 2.43 for PCR by Abbott when the costs are extended to a year.
It can be demonstrated that if XpertHIV was used instead of PCR by Abbott, the Government of Malawi would save resources because of two factors: 1) lower cost of XpertHIV test and 2) higher return rate of results for XpertHIV. We can examine two scenarios, one in which both testing strategies operated at observed efficiency and the other in which they operated at full capacity. Each year approximately 40,000 HIV-exposed infants are born in Malawi who are eligible for testing. In 2018, 38,393 HIV-exposed babies were born & discharged from maternity units in Malawi. The MoH collected and recorded 45,637 DNA-PCR samples. Of these, 31730 (70%) results were returned to collection sites. However, only 20038 (44%) mothers received their infants’ results. Therefore in 2018, the MoH spent $3,041,960.97 ($66.66 per test for 45,637 samples) given the observed efficiency scenario. However, if XpertHIV was used, MOH would have spent $1,932,300.57 ($42.37 per test for 45,637 samples) and saved $1,109,660.40. Considering that 56% of the samples (25,599) were not received by mothers/guardians of the infants, then $1,083,878.48 was lost. Assuming the best case scenario that XpertHIV has a 100% results return rate, the savings from implementing XpertHIV would be as high as $2,193,538.88. Assuming the full capacity scenario, 45,637 DNA-PCR samples would have cost $1,234,937 ($27.06 per test for 45,637 samples) for PCR by Abbott. If XpertHIV was used, MoH would have spent $735,668 (($16.12 per test for 45,637 samples) and saved $499,269 on PCR. For the samples that were not received by mothers/guardians, $692,709 was lost. So XpertHIV would have saved a total of $1,191,978, assuming XpertHIV had a 100% results return rate.
Table 5 shows the characteristics of respondents to the household cost survey. Of the 200 participants recruited for the household cost survey, their caregivers were 2% male and 98% female. 21% of the carers were accompanied by someone. Most (59%) of the guardians were housewives; 60% of the guardians walked to the hospital and the mean time to travel to the hospital was 1.7 hours. About 90% of the sampled children were outpatients, while 10% were inpatients. The mean length of stay for the inpatients was 5.06 days with a maximum of 21 days.
Table 6 presents the results of the household cost survey. The total economic cost that guardians incurred was $1,719. Guardian time and guardian’s companion’s time waiting for their child to get care were the most significant contributors to the total cost at $550.83 and $357.33. Guardian’s inpatient time was the third-highest contributor at $253.89. There were no reported expenditures against consultation, registration, laboratory test, medicines, gifts to health workers and under-the-table payments. From the patient perspective, the cost per test was $2.45.
Cost-effectiveness
For the cost-effectiveness of XpertHIV vs PCR by Abbott, we assumed that clients always need test results immediately and that the cost-effective strategy reduces the cost per hour of waiting for results. Table 7 shows the base case cost-effectiveness results. XpertHIV was more cost-effective than Abbot PCR because of the lower mean cost per test ($42.34) and lower turn-around time (146.05h). The incremental cost-effectiveness ratio is, therefore, $0.17/h reduced.
Sensitivity analysis
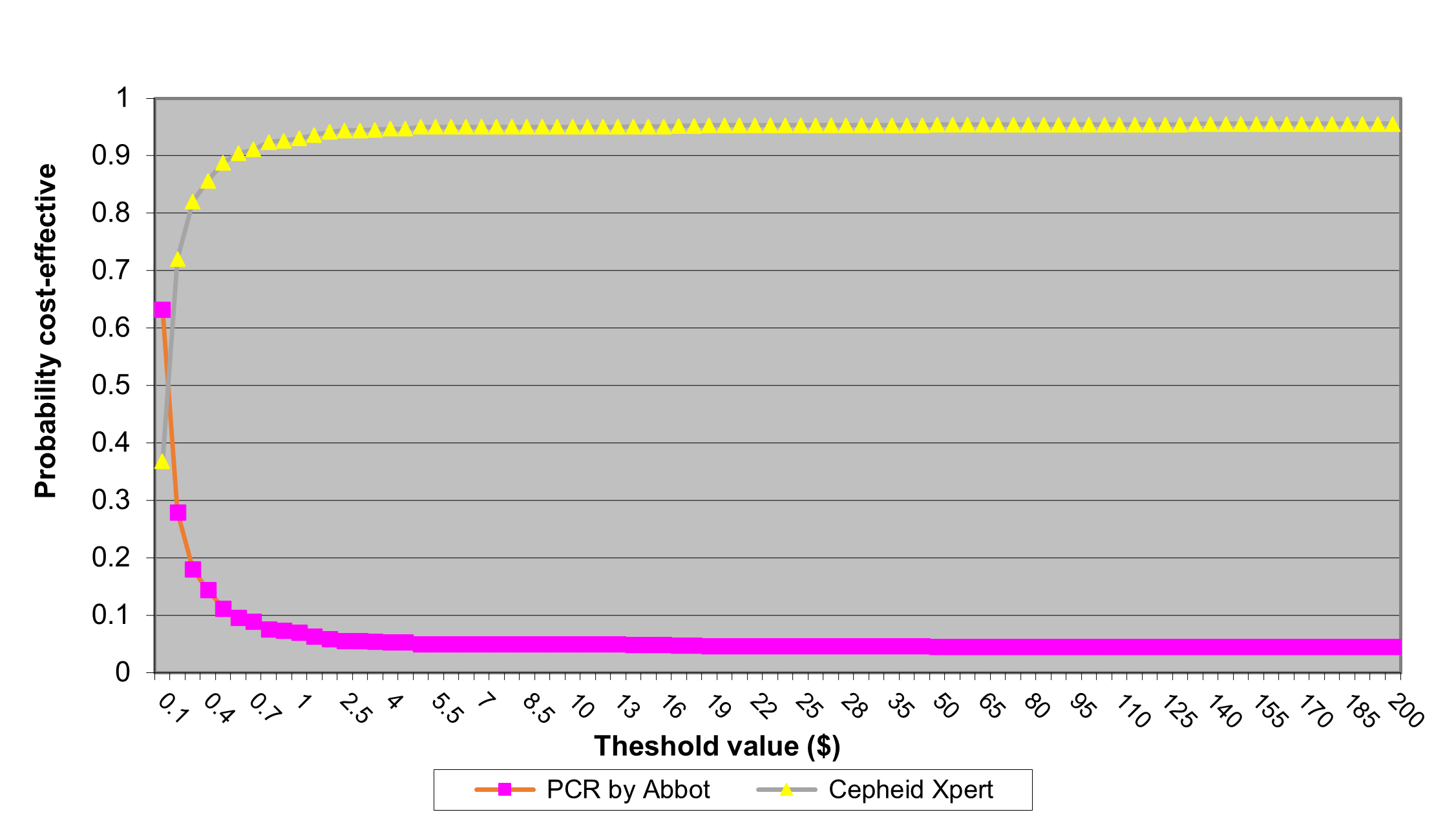
Figure 1 shows the cost-effectiveness acceptability curves from the probabilistic sensitivity analysis. When the threshold willingness to pay for an hour waiting for results was less than .$0.20, PCR by Abbot had a higher probability of being cost-effective. For threshold values greater than $0.20, XpertHIV had a higher probability of being cost-effective, from $0.70, the probability of XperHIV being cost-effective was greater than 0.9.

Discussion
XpertHIV was cost-minimising at $42.34 per test compared to $66.66 for PCR. Over a year, we extrapolated that XpertHIV remained cost-minimising at $16.12 compared to PCR at $27.06. Cost-minimisation of XpertHIV would derive from its relatively high results return rate and lower cost than Abbot PCR. From the patient perspective (travel, food, lost productivity), the cost per test of XpertHIV was $2.45. XpertHIV had a mean TAT of 7.10 hours compared to 153.15 hours for PCR.
The findings of this study are similar to other studies in Africa, where the cost per test result returned within 30 days in 8 countries was less for POC (US$27·24, range $21·39 - $33·10) than conventional PCR testing ($131·02, $96·26- $165·76)30 and $32.65 for POC,31 $30 (testing once) to $55 (testing twice),32 $24.18 for conventional and $27·61 for POC.33
When costs were extrapolated to a year, XpertHIV remained cost-minimising because of its higher throughput and the assumption of the machine being used at full capacity every day. These findings are similar to a South African study which demonstrated that higher volume facilities had better instrument utilisation and consequently lower POC costs.34 XpertHIV had a higher probability of being cost-effective for all willingness to pay (WTP) values that were simulated. Although there is no official Government of Malawi WTP threshold for reduced time accessing health care, the CEACs in Figure 1 show that whatever threshold value may be estimated, XpertHIV would probably still be a cost-effective strategy relative to PCR.
According to probabilistic sensitivity analysis results, XpertHIV had a higher probability of being cost-effective for all willingness to pay (WTP) thresholds that were simulated. Although there is no official Government of Malawi WTP threshold for reduced time accessing health care, the CEACs in Figure 1 show that whatever threshold value may be estimated, XpertHIV would still be a cost-effective strategy relative to PCR.
Before this costing and cost-effectiveness analysis, we conducted a feasibility study evaluating the performance of XpertHIV, which was found to be as sensitive and specific as PCR by Abbott and much easier to use compared to the standard EID strategies using PCR by Abbott systems in Malawi.17,18 XpertHIV was also accepted by parents and caregivers as a POCT for EID.19,20 Therefore, comparing costs of current practice and the XpertHIV was necessary before recommending its use for EID.
The study had several limitations. First, it was conducted in only one site, so there was no cost variation by geography or facility level. Using this assay outside of the study setting or a health centre may result in different findings as costs may vary in different directions. This may be due to several operational factors including GeneXpert machines of different capacities at health facilities and different levels of their utilisation/idle capacity. For example, Mulanje District Hospital had a VXI module Cepheid GeneXpert machine, which allows 96 tests to be performed per day, while other districts have IV module Cepheid GeneXpert machines which allow a maximum of 21 tests per day. And the machine at Mulanje District Hospital never runs at full capacity. However, more recently, HPV, Covid-19 and TB tests are run concurrently. It may thus be worth extending this study to consider this scenario in future. Also, if this study was conducted in the districts with lower capacity machines eg 4 module Cepheid Genexpert platforms, TAT would have been higher.
In this analysis, we priotised TAT because it impacts time to ART initiation. The study did not follow up patients over time to link how turnaround times may subsequently have affected health outcomes of the children. There is a need for implementation studies to assess the impact of the transition to POCT, to continue to monitor the impact on ART uptake, survival, and broader outcomes such as Quality Adjusted Life Years or Disability Adjusted Life Years (DALYs ) which will in turn inform future cost effectiveness models. It will be important to extend this work to look at final outcome measures for Malawi or similar settings. According to the CHER trial conducted in South Africa, early initiation of ART is capable of reducing infant mortality from 16% to 4% decreasing of early infant mortality by 76% and HIV progression by 75%.6
The most significant impact of this study and contribution to the policy was that by 2019, XpertHIV using DBS is implemented and now rolled out in Malawi for EID and Viral load monitoring. The already existing Cepheid platforms are used for HIV EID and Viral load monitoring, which has improved TAT and loss to follow-up of HIV-exposed infants. Furthermore, XpertHIV EID testing is concurrently being undertaken together with TB, HPV and Covid-19 testing, demonstrating better instrument utilisation of the Cepheid GeneXpert platforms and high throughput.
Conclusion
This study conducted a costing and outcomes analysis of POCT XpertHIV and PCR by Abbott Systems. Results showed that XpertHIV cost was $42.34 per test compared to $66.66 for PCR by Abbott. When the results of the study were extrapolated from the study period (29 days) to a year (240 working days), XpertHIV remained cost-minimising at $16.12 compared to PCR by Abbott at $27.06, and the median TAT for results was 7.10 hours for XpertHIV compared to 153.15 hours for PCR. Therefore, XpertHIV is cost-effective. Implementing XpertHIV in Mulanje district could significantly improve EID, decrease follow-up loss and reduce morbidity and mortality. More extensive modelling needs to determine the full and long-term consequences of implementing XpertHIV in Malawi and sub-Saharan Africa.
Funding Statement
Part of this work was funded by Aldama Foundation and sponsored by McClay Foundation, 20 Seagoe Industrial Estate, Craigavon, Belfast, Northern Ireland. BT63 5QD which covered the cost of the Cepheid Xpert HIV-1 Qual cartridges, PCR by Abbott M2000 and staff who undertook the study between July and August 2018. Dr. Nyirenda-Nyang’wa was partially supported one day/week from January 2019 to June 2020 by the Fogarty International Center-funded Malawi HIV implementation Research Scientist Training program (D43 TW010060).
Author Contribution
Conceptualisation: MNN, DA. Data cleaning: MNN, PC, DN, GM. Methodology and Formal analysis: MNN, MA, DN, PC, GM. Project administration: MNN. Supervision: GM, MA, DN, JC. Writing – original draft: MNN, GM. Writing – review & editing: MNN, GM, MA, DN, JC, PC, CM, MC, KM, NK, DF, VM, MH, HCM, NK, DA, AO.
Acknowledgements
The authors would like to thank Professor Paul Revill, who reviewed the paper, for his helpful comments. The authors are also grateful to all the participants and their caregivers for consenting to participate in this study; We also acknowledge the contribution of the staff of Mulanje District Hospital, especially the laboratory staff: Christina Kaliwo, Thei Chide, Connex Chisuwo, Laston Banda, Sangwani Mkandawire, Joseph Limbani , Rebecca Thukuwa , Dennie Goster ; the Deputy District Hospital Officer Martin Malunga; HIV DETECT study team - research nurses Linley Mlozeni and Ida Nkhonjera, health surveillance assistants for their support in recruitment of participants; District Hospital Officer and Ministry of Health, especially the Director of Diagnostic Mr James Kandulu.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Conflict of interest
The authors completed the Unified Competing Interest form (available upon request from the corresponding author) and declare no conflicts of interest.
Research Involving Human Participants
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.