

Introduction
Visceral leishmaniasis (VL) is present in 12 countries on the American continent, with 97% of the cases reported in Brazil with an incidence rate of 2.0 per 100,000 inhabitants and a fatality rate of around 7%.1 The etiological agent in the Americas is the protozoan Leishmania infantum, which is transmitted by the phlebotomine Lutzomyia longipalpis, with dogs serving as the main reservoir in the urban environments.2
Climate and socioeconomic changes were suggested to have a role in the expansion of VL.3 Several studies have already investigated the relationship between the distribution and expansion of the disease with socioeconomic factors, indicating a strong relationship between VL and less favoured locations with low income and poor infrastructure.4–6 There is growing evidence of the climate change impact on vector-borne diseases.7–11 For example, changes in temperature and humidity, especially in endemic areas of the disease, can aggravate leishmaniasis, as these changes are directly linked to the natural cycle of the disease and the vector’s ability to survive.12,13 The present study investigates the hypothesis that climatic factors are responsible for the variation of VL cases, with the prediction that warmer and wetter climates may have contributed to increased cases over the last decades. We tested this hypothesis in an endemic area of the disease in Brazil, using reliable data from the last three decades.
Methods
Ethics
This study was approved by the Research Ethics Committee of the Federal University of Ouro Preto (Report No. 3,291,628) and by the Ethics Committee of the Municipality of Belo Horizonte (Report No. 3,343,825).
Study design
This was a time-series study of VL carried out in the city of Belo Horizonte, capital of the state of Minas Gerais, in the southeastern region of Brazil. It is Brazil’s sixth most populous city, with an area of 331,354 km². It is located 860 meters above sea level and has an estimated population of 2,521,564 in 2020. It presents dry winters and rainy summers with a predominantly tropical climate.
All known VL cases of residents in the municipality in the period from 1994 to 2019, confirmed by the Epidemiological Surveillance sector of the Municipal Health Department, were included. Confirmed cases were those with at least one positive laboratory diagnostic test. The environmental variables, average temperature, maximum temperature, minimum temperature, the maximum and minimum temperature in the dry and rainy seasons, total precipitation, number of rainy days, precipitation in the dry and rainy seasons, and the relationship between precipitation and rainy days were obtained from the National Institute of Meteorology.14 As we used the annual data, monthly fluctuations were not assessed.
Data analysis
The incidence of VL along the time series was initially described through the absolute number of cases and relative frequency per 100,000 inhabitants. To calculate the incidence rate per year, the population estimates were obtained by the Instituto Brasileiro de Geografia e Estatística.15
The explanatory variables chosen to be tested were: total precipitation, the maximum and minimum temperature in dry and rainy seasons, number of rainy days, and precipitation/rainy days ratio. The correlation and collinearity between them were verified, and the following variables were excluded: average temperature, maximum and minimum temperature, and precipitation of dry and rainy periods. Next, a stepwise multiple linear regression was performed to test the effect of the remaining variables on the distribution of the number of cases (log-transformed to meet normal distribution requirements). Total annual precipitation was the only variable retained in the model, thus reduced to a simple linear regression model. All analyses were performed using Minitab 19 software, with significance set at P<0.05.
Results
Among the 1,897 cases in this study, the disease was the most common in children 1 to 4 years old (n = 344; 18.1%) and adults 40 to 49 years old (n = 249; 13.1%). Approximately 63% (n=1192) were men; in terms of the disease outcomes, 75% were completely cured (1,418), followed by 105 (5.5%) deaths and 374 (19.7%) censored cases.
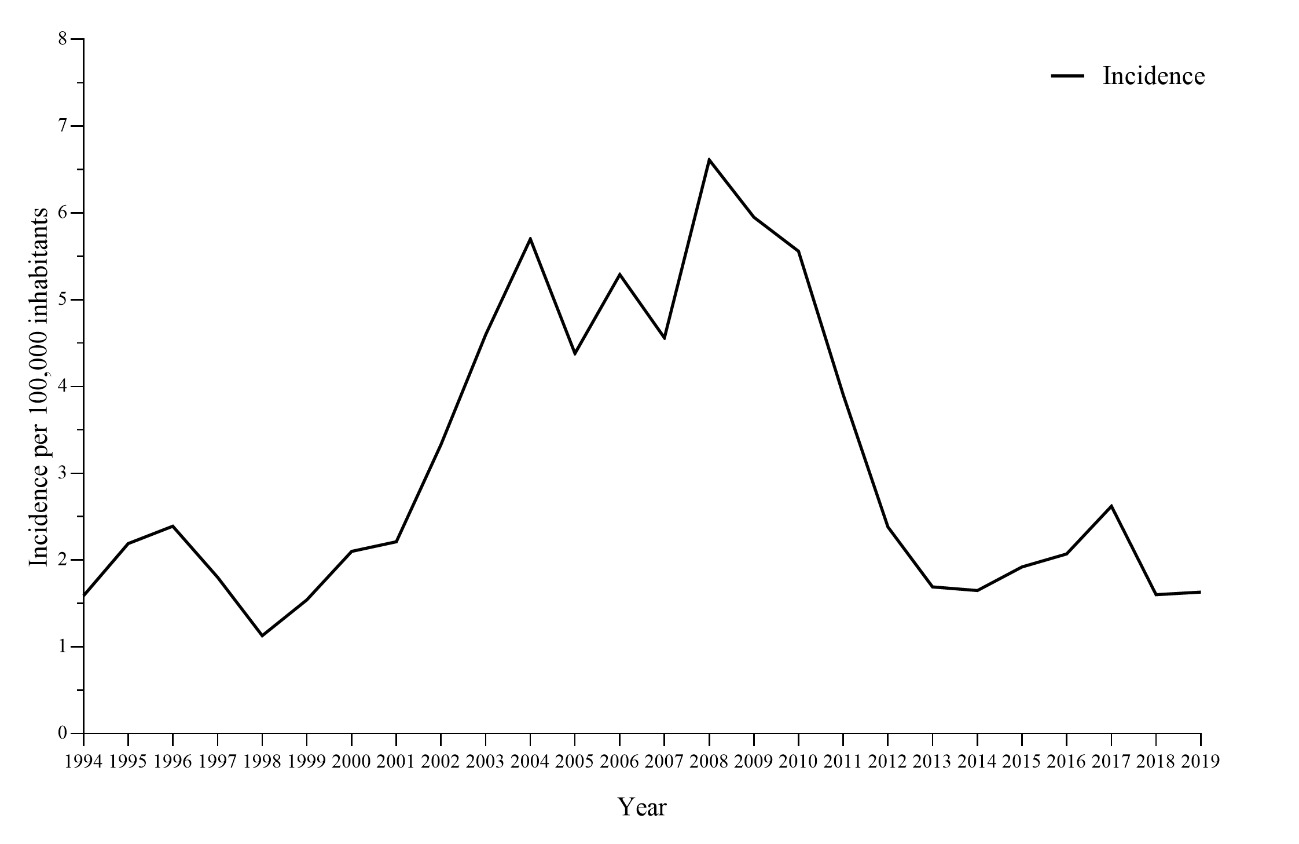
The first case reported in the city occurred in 1994, and there were substantial variations in the rates in the following years (Figure 1). In the 90s, the highest incidence rate was recorded in 1996 (2.39/100,000), followed by a decrease in the next years, with 1998 being the year with the lowest number of cases and incidence rate of the series. Noticeable increases in the number of cases occurred from 2003, leading to a peak in the number of cases in 2004. In the subsequent years, fluctuations in the number of cases were observed, but the series remained with high values. Another two peaks were observed, in 2006 and 2008, the latter with the highest number of cases (161) and incidence (5.08/100,000) recorded in the city’s history. Until 2010, the number of registered VL cases remained high, but in 2011 a significant decline was observed, with a slight increase in 2017. Still, values in 2017 were lower when compared to 2004 to 2010.
Climatic factors associated with the expansion of the disease
The variation in the number of VL cases during the study period showed a clear correspondence with total precipitation, increasing the infection burden in wetter years (Figure 2).

Indeed, yearly precipitation explained significantly the number of VL cases (F1;24 = 9,14, P = 0.006; Figure 3). Even along the period with less rainfall variation, between 1994 and 2005, with most of the years ranging from 1500 mm to 1600 mm, the two rainfall peaks, 1800 mm in 1995 and 1950 mm in 2004, resulted in increased numbers of VL cases. From 2001 onwards, an extremely accelerated increase in cases of the disease was observed, and from 2003 it started to follow the rainfall variation tightly, until a severe decline along with rain decline starting in 2010 until 2014, followed by a subtle increase of both in the next years.

Discussion
In the last three decades, there has been a considerable fluctuation in the number of VL cases in Belo Horizonte. It was evidenced that the rainfall partially drives the number of disease cases.
A recently published systematic review showed that socioeconomic, environmental and climate variables were associated with disease incidence in vulnerable human populations of arid and tropical developing regions. In addition, socioeconomic and climatic changes usually play a significant role in the presence and distribution of the disease.3 Several studies have already investigated the relationship between the distribution and expansion of the disease with socioeconomic changes, indicating a strong relationship with VL.6,16 Currently, new evidence is emerging relating to the impact of climate on vector-borne diseases.9,10 In this study, we found that total precipitation partially explained the variation in the number of cases, an important factor in the spread of the disease.
Previous studies showed that temperature and rainfall are fundamental factors for spreading this disease.9,17,18 Studies conducted in Brazil showed an association between VL incidence and annual precipitation.18–20 The effects of rainfall in the growing number of VL cases might be related to the vector’s transmission cycle, as the phlebotomine needs high temperature and humidity to reproduce.21
Precipitation drives the availability of nutrients for larval development and the suitability of the environment for reproduction.22–24 Therefore, environmental disturbances caused by the flooding of urban rivers, trash accumulation due to flash floods, and sewage overflow, particularly in areas under poor sanitarian conditions, may be neglected causes of VL outbreaks in very rainy years. Although the yearly rainfall is not as high as around 2008-2011, the rain regime has changed, and the city is experiencing more rain volumes and storms per rainy day than before.25 Such years need close monitoring, as disruptive rains could exacerbate epidemiologic scenarios, especially with Brazil returning to a situation of great populations experiencing extreme poverty.26 Poverty and poor infrastructure are already known to affect the presence of VL. A study in Belo Horizonte identified a relationship between income and education indices with the risk of VL infection.27
It is already established in the literature that several vectors, phlebotomine species, have activities such as biting and mating impacted by the climate.28 As identified in the present study, precipitation is associated with an increase in the number of cases, and the study carried out by Rajesh & Sanjay demonstrated an association between rainy periods and the presence of large numbers of sandflies.12 With the increase in the number of vectors, consequently, there is an increase in the number of cases in endemic areas. Many studies indicate that temperature as a variable correlated with VL.17,29,30 The temperature also affects the insect’s metabolism, so defecation, oviposition, and developmental stage changes are much slower at low temperatures.31 Besides a sufficient correlation between hot days and rainy days, after 2007, the region where Belo Horizonte is located has experienced high temperatures both in summer and winter.11 These continuously hot years may undermine any possibility of detecting a quantitative effect of temperature in the cases.
In addition to climate issues, a study in the city determined that from 1993 to 2007, VL showed a tendency to grow, probably due to the discontinuity of control programs and the delay in removing seropositive dogs. It also associates the form of urban space occupation as an influence in the risk of cases.32 According to Morais et al, the use of one information system to assess control actions may have contributed to an improvement in the effectiveness of activities leading to a reduction in canine seroprevalence and the incidence of human cases in the years 2008 to 2011.33 Although another work carried out in the municipality shows that the surveillance and control program was not very effective in reducing incidence rates, it emphasizes that if this did not exist, the epidemiological situation could be even more serious.34
A possible limitation of our study was the changes in VL diagnostic methods over the period evaluated. VL diagnosis is performed through a combination of clinical criteria, parasitological and serological tests. Bone marrow aspirate parasitological tests, immunofluorescence test (IFAT) and rapid diagnostic tests (RDT) are the main tests performed in Brazil.35 Throughout the historical series, new tests with greater sensitivity and specificity were introduced.36 However, these changes may have little impact on the data presented since the cases are not diagnosed by active search in epidemiological surveys, as in canine visceral leishmaniasis, but by demand when the patient seeks the health unit with clinical manifestations of the disease that are later confirmed in the laboratory.
The historical series evaluated demonstrates the endemicity of the disease and indicates the possibility that new epidemic periods of the disease may occur. Climate issues can influence these outbreaks.3 Extreme climate and poverty may interact more intensively in years under high rain volume, leading to an increase in VL cases. Thus, the use of meteorological data for epidemiological surveillance can contribute to better planning of their actions, intensifying interventions in periods and years of greater rainfall, avoiding an increase in the number of vectors and consequently in cases of the disease.
Ethics approval
The study was approved by the Ethics Research Committee of the Universidade Federal de Ouro Preto (protocol number 11980919.5.0000.5150).
Funding
This study was supported by the CNPq/BR/grant 407195/2021-1. ABR, SPR and MC are grateful to the CNPq for fellowships. The CAPES sponsored RVD scholarships (Programa de Pós-Graduação em Ciências Biológicas, Universidade Federal de Ouro Preto). The funders had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Author’s contributions
Rafael Vieira Duarte: Validation, Investigation, Formal analysis, Writing – original Draft, Writing – review & editing. Josefa Clara Lafuente Monteiro: Investigation, Writing – original Draft, Writing – review & editing. Tamara Coelho Cruz: Investigation, Writing – original Draft, Writing – review & editing. Lucas Moreira Ribeiro: Investigation, Writing – original Draft, Writing – review & editing. Maria Helena Franco Morais: Validation, Writing – review & editing. Mariângela Carneiro: Writing – review & editing. Alexandre Barbosa Reis: Writing – review & editing. Sérvio Pontes Ribeiro: Conceptualization, Methodology, Resources, Writing – review & editing, Supervision, Funding acquisition. Wendel Coura-Vital: Conceptualization, Resources, Writing – review & editing, Supervision, Funding acquisition.
Conflict of interest
The authors completed the Unified Competing Interest form (available upon request from the corresponding author) and declare no conflicts of interest.
Correspondence
Wendel Coura-Vital, PhD, Laboratório de Epidemiologia das Doenças Parasitárias e Infecciosas, Departamento de Análises Clínicas, Escola de Farmácia, Universidade Federal de Ouro Preto, Ouro Preto, Minas Gerais, Brasil, CEP 35400-000, phone: +553135591835; wendelcoura@ufop.edu.br