Introduction
By December 2020, one year after the first reported COVID-19 case in China,1 50 countries had already started their vaccination against COVID-19.2 Globally, as many as 194 COVID-19 vaccines were in the pre-clinical development, and 137 COVID-19 vaccines were in clinical trials.3 Of these, 21 vaccines are currently in use, 10 of which are approved for use by the WHO.4 As of 26 January 2021, over 9.7 billion vaccine doses have been administered worldwide.5
Nonetheless, access to COVID-19 vaccines is far from equitable.6 There is a clear gap in the delivery and administration of vaccines between high and low or middle-income countries. About 67.5% of populations have been vaccinated with at least one dose in high-income countries. As opposed to about 11% of populations in low-income countries.6 According to WHO, 56 countries are being excluded from the global vaccine marketplace, most of them in Africa.7 The gap is also due to the significant financial burden in low-income countries, which would need to increase their health expenditure by 30-60% to vaccinate 70% of their population.6 This gap will leave low and middle-income countries more vulnerable to COVID-19 spread, new surges of the virus’s variants, and a slower ability to recover from the crisis.
COVID-19 Response in Lebanon
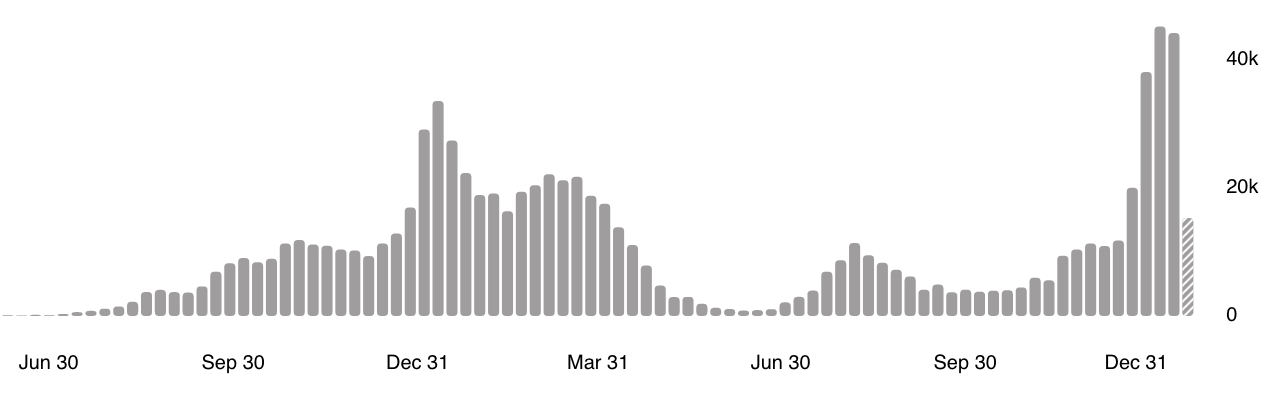
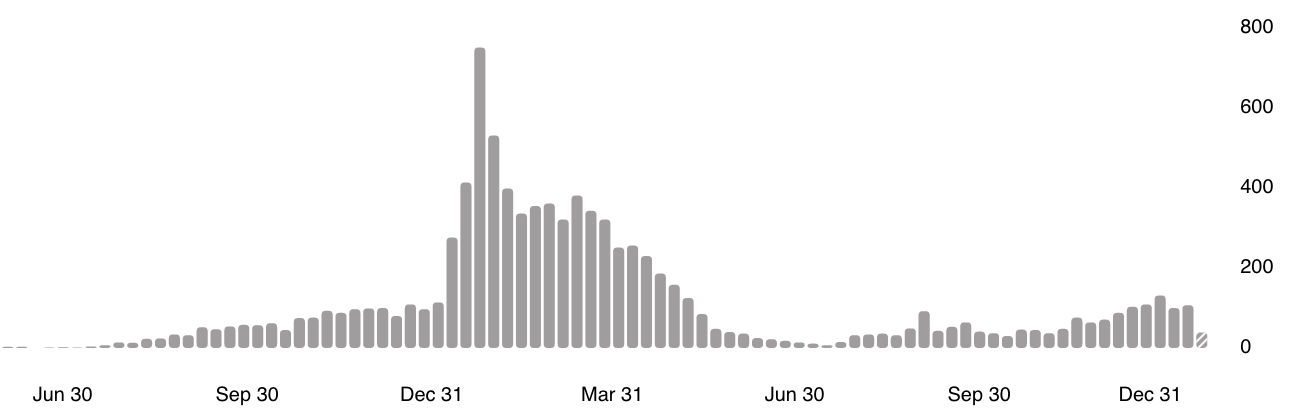
The Lebanese government initiated a quick response after reporting the first COVID-19 case in the country in February 2020. It quickly applied strict containment measures (i.e. halting flights, closing schools, and imposing lockdown measures).8 However, the overall capacity to respond to the pandemic was constrained by the already weak healthcare system, coupled with an economic crisis, currency devaluation, and political instability in Lebanon.9 Furthermore, the massive Beirut blast in August 2020, which amounted to over 6,000 injuries and 200 deaths, added to the fragility of both country and the healthcare system.9 The blast has damaged many hospitals and shifted resources to deal with this emergency. As a result, the remaining hospitals were overcrowded, exacerbating Lebanon’s political and financial crises and reducing efforts to control the pandemic.10 As of 3 January 2021, there has been over 874,000 cumulative cases of COVID-19 in Lebanon and 9,513 COVID-19 deaths.11
__109027_.png)
__109027_.png)
The poor living conditions for refugee populations in Lebanon make them more susceptible to COVID-19 spread.12 Lebanon is the country with the largest number of refugees per capita globally, with an estimated 1.5 million Syrian refugees13 and 480,000 registered Palestinian refugees.14 These refugees suffer from high levels of poverty, unemployment, and poor housing conditions in overcrowded refugee camps and urban areas.14,15 Palestinian refugees are barred from working in as many as 39 professions.14 Only registered Syrian refugees can work in Lebanon in only three sectors; construction, environment and agriculture.16 A 2020 United Nations report states that nine out of ten Syrian refugees in Lebanon live in extreme poverty.17 The same report indicates that the multi-crisis situation in Lebanon has hit vulnerable populations, including refugees, the hardest.17
According to the United Nations High Commissioner for Refugees (UNHCR), as of January 2021, there has been 2,734 cumulative COVID-19 cases among registered refugees in Lebanon.18 The United Nations Relief and Work Agencies for Palestine Refugees (UNRWA) has reported 3,614 cumulative COVID-19 cases amongst Palestinian refugees in Lebanon as of 31 December 2020.19 However, there has been no data on reported COVID-19 cases by UNHCR and UNRWA beyond these dates, which could be due to under-reporting, under-testing, and/or a lack of efforts to prioritise such data representation. Moreover, the MoPH data on COVID-19 is not segregated by nationality. This raises questions on the inclusion of refugee populations in national plans and reporting mechanisms and the lack of coordination between refugee UN agencies and the Lebanese government.
Vaccine Equity in Lebanon
The Ministry of Public Health (MoPH) 's vaccine roll-out strategy in January 2021 stated that procurement plans for about 6.33 million vaccine doses had been secured.20 The Ministry of Public Health announced in January 2021 that 80% of the population in Lebanon (about 5.42 million people) would be vaccinated by the end of 2021.21 In late October 2021, over nine months after his announcement, about 3.4 million vaccine doses were administered, of which 1.58 million were second doses.22 This means that only 23.4% of the population in Lebanon have been fully vaccinated, and the government is far from reaching the 80% target. Other factors hampering the implementation of vaccination plans include delayed shipments from suppliers, electricity cuts, and internet issues that affect the operation of registration services.23
There has been apparent inequity in administering vaccine doses in Lebanon between nationals and migrant populations. About 89% of vaccine doses have been administered to the Lebanese population, while only 5.26% have been administered to registered refugees (2.96% to Syrian refugees and 2.3% to Palestinian refugees).24 Even though the percentage of the Lebanese population is the largest in Lebanon, Syrian (registered and unregistered) and Palestinian refugees still represent a notable proportion (30%) of the population of Lebanon.13
Fear of detention or deportation, and mistrust in the Lebanese government are possible reasons why many refugees do not register through the government’s vaccine platform. Many Syrian refugees interviewed by Human Rights Watch mentioned that they fear being detained or deported from Lebanon if they register because of not having a legal residency in Lebanon.25 About 70% of Syrian are not legal residents in Lebanon, mainly due to strict civil documentation requirements that are challenging to obtain.18 Moreover, Palestinian refugees expressed their mistrust of the Lebanese authorities due to the long-standing systemic discrimination against them.25 Some Palestinian refugees expressed to Human Rights Watch that they fear registering for the vaccine and not receiving it in the end or having to pay expensive fees that they cannot afford.25
The demographic and geographical distribution of refugees in Lebanon also calls for intensified vaccination roll-out. Even though 56% of registered Syrian refugees are children,13 vaccination plans in Lebanon target all people above age 11,24 which means that plans should still cover a good proportion of the Syrian refugee population. Over 23% of registered Syrian refugees live in the governorates of Beirut and Mount Lebanon,13 which have over 46% of COVID-19 cases in Lebanon.26 Over 60% of vaccines in the country were administered in Beirut and Mount Lebanon, while most Syrian refugees there remain unvaccinated.
There has been a lack of implementation plans and a slow response regarding securing and distributing vaccines in Lebanon on the political level.27 A clear division of roles between the MoPH and other health actors on the ground is absent. Government and health officials have shared contradictory information regarding vaccine distribution to refugee populations. Some stated that all those living in Lebanon would be targeted regardless of their nationality,21 while another politician indicated that UN agencies (UNHCR and UNRWA) are responsible for ensuring the vaccination of refugee populations in Lebanon.28 The MoPH vaccine roll-out strategy29 does not mention migrant or refugee populations and does not explicitly include them in the priority groups selected to be first vaccinated.
Policy Recommendations & Conclusion
The Lebanese government and MoPH must intensify efforts for a quick procurement, delivery and administration of vaccinations. Clear national plans must be in place whereby state and non-state actors collaborate and are aware of their specific roles in a national and equitable COVID-19 response. Prioritisation of need-based distribution of vaccines nationally for all the population would help the country out of the pandemic crisis. This will not be achieved if migrant populations and refugees are neglected from the national vaccine plan. The needs, risks and vulnerabilities of refugee populations in Lebanon must be considered in all national public health plans, including COVID-19 vaccination.
Community-led awareness campaigns can help to increase national vaccine efforts. These can inform refugees on the available national services for COVID-19 how to register and reach these services. On the other hand, the Lebanese authorities should facilitate vaccinations regardless of people’s residency status and permit vaccinations without requesting identity documents. This would re-assure migrants who are not legal residents in Lebanon, and support their access to vaccinations.
The Lebanese authorities must respect its national and international duty to protect the health of all its residents, including vulnerable populations. The United Nations Security Council’s Resolution 2565 (2021)30 calls for national and international efforts to facilitate equitable access to vaccines in post-conflict situations and complex humanitarian emergencies. The resolution also includes the most vulnerable populations in national COVID-19 plans, such as refugees, internally displaced people, migrants, and stateless people.30
Finally, consolidated plans for re-establishing a sustainable and equitable health system are required in Lebanon. These can be achieved through the prioritisation of prevention initiatives and need-based fund allocations. It is essential to tackle the root causes of the health system fragility in Lebanon and acknowledge the existing multi-crisis situation. The new government in Lebanon must collaboratively set robust plans to exit the financial crisis and aid dependence.
Ethics
No ethics approval was needed for the writing of this article.
Acknowledgment
This paper is part of a political economy of health special issue, facilitated by the Global Health Institute (GHI) at the American University of Beirut (AUB), and Research for Health in Conflict in the Middle East and North Africa (R4HC-MENA) consortium.
Funding
The publication fees of this articles are funded by the Global Health Institute (GHI) at the American University of Beirut (AUB) and the UK Research and Innovation GCRF Research for Health in Conflict in the Middle East and North Africa (R4HC-MENA) project: developing capability, partnerships and research in the Middle and North Africa ES/P010962/1.
Authorship contribution
Both authors contributed to the conception, drafting and writing of the article. Both authors provided critical feedback on the manuscript and have agreed to be accountable for all aspects of the work.
Conflict of interest
The authors completed the ICMJE Unified Competing Interest form at (available upon request from the corresponding author), and declare no conflicts of interest.
Correspondence
Rasha Kaloti
Research associate of the Global Health Institute at the American University of Beirut
rk216@aub.edu.lb