Background
South Africa’s population was 58.78 million people in 2019. It is an upper-middle-income country with a gross domestic product (GDP) of International Dollars (Int$) 761.82 billion,1 per capita GDP of Int$ 12,961.71 and inequality-adjusted human development index of 0.468 in 2019.2
In the same year, the country had a total of 26,587,883 disability-adjusted life-years (DALYs) from all causes.3 Out of which, 50% were from communicable, maternal, neonatal, and nutritional diseases (CMNND); 38% from non-communicable diseases (NCD); and 12% from injuries (INJ).3
The persistent, significant loss in DALYs has been attributed to the sub-optimal performance of three sets of systems. First, the national,4–6 district,7,8 and community health system responsible for assuring affordable access to quality health services.9,10 Rispel et al. uncovered human resources for health gaps and weaknesses that ought to be addressed to ensure a high performing health system.10 According to the WHO World Statistics 2020, the universal health coverage (UHC) service coverage index for South Africa was 69% in 2017, which implied a 31% service coverage gap.11 The index encompasses reproductive, maternal, newborn and child health, infectious diseases, and non-communicable diseases service capacities and access. About 384,300 (1.4%) of South Africans had household expenditures on health greater than 10% of total household expenditure or incomes, and 27,450 (0.1%) had household expenditures on health greater than 25% of total household expenditure or incomes in 2017.11
Second, the systems addressing social determinants of health, including food, education, water, sanitation, shelter (dwelling) and physical security.12 About 27% of children under the age of five were stunted, 2.5% were wasted, and 13.3% were overweight in 2017.11 Approximately 5.6% of adults aged 15 years and older are illiterate, and 24% have no secondary school education.12 Seven per cent of the population were not using improved drinking water sources, and 34% were not using improved sanitation.13 Around 79% of households live in a formal dwelling, 14% in informal dwelling, 6% in traditional dwelling and 1% in other dwellings.14 The community reported 1,662,815 serious crimes between 1st April 2017 to 31st March 2018. About 29% of crimes occurred in Gauteng, 21% in Western Cape, 15% in Kwazulu-Natal, 10% in Eastern Cape, 6% in Mpumalanga, 6% in North-West, 6% in Limpopo, 5% in Free State and 2% in Northern Cape.15
Finally, the national health research system is meant to produce high-quality contextualized knowledge and promote its use in developing resilient and sustainable systems to promote population health.16 Senkubuge et al. estimated the overall NHRS barometer score of South Africa to be 84%, implying a performance deficit of 16%.17 The authors recommended actions needed to bridge deficits in NHRS financing and human plus physical resources.17
The sub-optimal performance of the national health system may partially be associated with the fact that current health expenditures (CHE) per capita for South Africa of $471 is less than the US$536 per person recommended for the attainment of United Nations (UN) Sustainable Development Goal 3 (SDG3).18,19 Stenberg et al. also recommended that about 60% of CHE per person consist of general government expenditure on health. There is a need for advocacy for increased government investment in the health system and other systems that address social determinants of health12; improved equity in health and health-related spending20,21; and efficient use of health development resources.22–24
Monetary valuations of health losses have been estimated and used in Africa,25–28 Asia,29–32 Eastern Mediterranean,33–35 European,36–41 North American,42–45 and South American countries to advocate for increased investments into health development.46–49 To date, no study has estimated the dollar value of DALYs lost from a wide range of diseases and conditions in South Africa. Thus, this study aims to contribute to bridging the existing knowledge gap.
The specific objectives were: (a) to estimate the dollar value of DALYs lost in South Africa in 2019; and (b) to forecast the reductions in the dollar value of DALY losses assuming some specific SDG 3 targets are attained by 2030.
Methods
Study area and disease categories
The study reported in this paper centres on the International Dollar (or Purchasing Power Parity) valuation of the 26.6 million DALYs from 157 causes in South Africa in 2019.3 Its scope included three disease clusters. First, the CMNND cluster comprised 24 infectious and parasitic diseases, three respiratory infections, maternal disorders, neonatal disorders, and five nutritional deficiencies. Second, the NCD cluster consisted of 30 neoplasms, three diabetes and kidney diseases, ten mental disorders, two substance use disorders, seven neurological disorders, three sense organ disorders, 11 cardiovascular diseases, five chronic respiratory diseases, ten digestive diseases, three sense organ diseases, 12 skin and subcutaneous diseases, six musculoskeletal diseases, seven other NCDs (congenital disabilities; urinary diseases and male infertility; gynaecological diseases; haemoglobinopathies and haemolytic anaemias; endocrine, metabolic, blood, and immune disorders; oral disorders; sudden infant death syndrome).3 Third, the injuries cluster consisted of 17 causes, including two transport injuries, 11 unintentional injuries, and four self-harm and interpersonal violence.3
The DALY is a sum of years of life lost (YLL) due to premature mortality in the population and the years of life lost to disability (YLD) for people living with a health condition.50 The YLD is obtained by multiplying disability weights by the number of years lived in a specific health state. The Institute for Health Metrics and Evaluation (IHME) GBD 2019 Diseases and Injuries Collaborators article describes methods and data sources used in 2019 DALY estimations.51
Estimation of the Dollar Value of DALY Lost in South Africa in 2019
The Organization for Economic Cooperation and Development (OECD) defines human capital (HC) as “The health (longevity and quality of life), knowledge, skills, competencies and attributes embodied in individuals that facilitate the creation of personal, social and economic wellbeing (p.18)”.52 There is a substantial body of evidence of a negative correlation between ill-health and risky health behaviours and educational achievement and academic performance.53,54 Poor health negatively affects educational outcomes by causing learning disabilities,55,56 eroding concentration,57–59 and reducing school attendance.60 Past research has revealed that good health has a statistically significant positive effect on the gross domestic product (GDP) or aggregate output.61,62
The study reported in this paper employed the HC approach (HCA) presented below to estimate the dollar value of DALYs from various causes. We chose to use HCA because of the availability of data on South Africa’s DALY per cause, current health expenditure per person, and GDP per person.
TDVD=(DVDCMNN+DVDNCD+DVDINJ)
As done in similar studies,63,64 DVD from each CMNN, NCD and INJ were estimated by multiplying the DALYs associated with different causes by South Africa’s 2019 GDP per capita (GDPPC) net of current health expenditure per person (CHEP). The DVD from jth cause (disease or injury) was estimated using the following formula:
DVDj=DALYj×(GDPPCINT$−CHEPINT$)
where: is the number of DALYs lost from jth disease or injury; GDPPCINT$ is the GDP per person (GDPPCINT$) in International Dollars (Int$) or Purchasing Power Parity; CHEPINT$ is the current health expenditure per person in International Dollars. A discount factor was not introduced in equation (2) since DALY estimates from the IHME global burden of disease database are already discounted at a rate of 3%.3
It is illustrated below how the dollar value of DALYs from road injuries (DVDRINJ) in 2019 was estimated using Equation 2. The DALYs from road injuries (DALYRINJ) were 1,051,493; GDPPCINT$ was Int$12,961.702; and CHEPINT$ was Int$ 1,170.098852 in 2019. Hence:
DVDRINJ=DALYRINJ×(GDPPCINT$−CHEPINT$)=1,051,493×⌊12961.702−1170.098852⌋=Int$12,398,792,099
Forecast of the Dollar Value of DALYs Lost in South Africa in 2030
The dollar value of forecast DALY losses in 2030 (MVDj2030) assumes achievement of the SDG3 targets in Table 1. Those targets include maternal mortality ratio (Target 3.1), neonatal mortality (Target 3.2), HIV/AIDS deaths (Target 3.3), tuberculosis (Target 3.3), malaria (Target 3.3), neglected tropical diseases (NTD) (Target 3.3), hepatitis (Target 3.3), NCD (Target 3.4), and injuries (Target 3.6).
The percentage reductions from baseline year (Y1) to the SDG deadline year of 2030 (Y2), which are contained in Column C of Table 1, were calculated using the following formula: ((Y2-Y1)/|Y1|) x 100. For instance, for road traffic injuries-related deaths (SDG3.6), percentage change from Y1=19,239 in 2019 to Y2=9,620 deaths in 2030 = ((9620 – 19239)/|19239|) x 100 = -50% change or 50 % decrease.
The anticipated dollar value of DALYs expected to accrue to South Africa in 2030 was estimated using the following equation28:
MVDj2030=MVDj2019−[MVDj2019×(SDGjER / 100)]
Where: is the total dollar value of DALY loss expected from jth health condition in 2030 assuming attainment of the related target; is the total dollar value of DALYs lost from jth health condition in the year 2019; and is the SDG jth health condition expected percentage reduction in mortality by 2030 contained in Table 1.28
As an example, it is demonstrated below how the dollar value of DALYs from RINJ in 2030 was appraised. The for South Africa in 2019 was Int$ 12,398,792,099, and SDG target 3.6 is to reduce the number of deaths from road injuries by 50% Thus:
MVDRINJ2030=MVDRINJ2019−[MVDRINJ2019 ×(SDGRINJ / 100)]=12,398,792,099−[12,398,792,099×(50100)]=Int$ 6,199,396,050
Estimation of Dollar Value of DALYs Losses Prevented by 2030
Following Kirigia and Mwabu28 and Muthuri and Kirigia,75 the dollar value of expected DALY losses likely to be prevented by ultimately achieving SDG3 target j (j = 3.1, 3.2, 3.3, 3.4, 3.6) contained in Table 1 was calculated using the following formula:
MVDSDG3j_Saving=[MVDj2019−MVDj2030]
For instance, the potential dollar value of DALYs saved by attaining SDG3 target 3.6 on road injuries was appraised as follows:
MVDSDG3.6Saving=[MVDRINJ2019−MVDj2030]=(12,398,792,099 −6,199,396,050)=Int$6,199,396,050
Data Sources and Analysis
The 2019 DALYs data estimates for the 157 causes for South Africa was from the Global Burden of Disease Collaborative Network database,3 and data on GDP per person in 2019 (Int$12,961.702) was from the International Monetary Fund (IMF) World Economic Outlook database.1 The projection of current health expenditure per capita (Int$1,170.098852) in 2019 used data from the WHO Global Health Expenditure Database.18 Since the CHEPC were Int$1,129.38391113 and Int$1,090.08569336 in 2018 and 2017,18 rate of change equals 0.0360505765825344 (3.60506%). Therefore, the CHEPC for 2019 equals Int$1,170.098852, i.e. Int$1129.38391113 + (Int$1129.38391113 x 0.0360505765825344). The net GDP per capita equals Int$11,791.6031476907, i.e. 12,961.702 minus 1,170.098852.
Equation (2) was estimated for each of the 157 causes (disease or injury) of DALY losses. In addition, equations (4) and (5) were calculated for SDG targets 3.1, 3.2, 3.3, 3.4 and 3.6. The seven equations developed in this methods section were analysed using Excel Software of Microsoft (New York).
Results
Estimates of Dollar Value of DALYs in South Africa in 2019
All causes: In 2019, South Africa incurred a total loss of 26.6 million DALYs from all causes valued at Int$313.5 billion. That is an average value of Int$ 11,791.6 per DALY. Out of the total value of DALYs, 50% accrued to CMNND, 38% to NCD, and 12% to INJ.
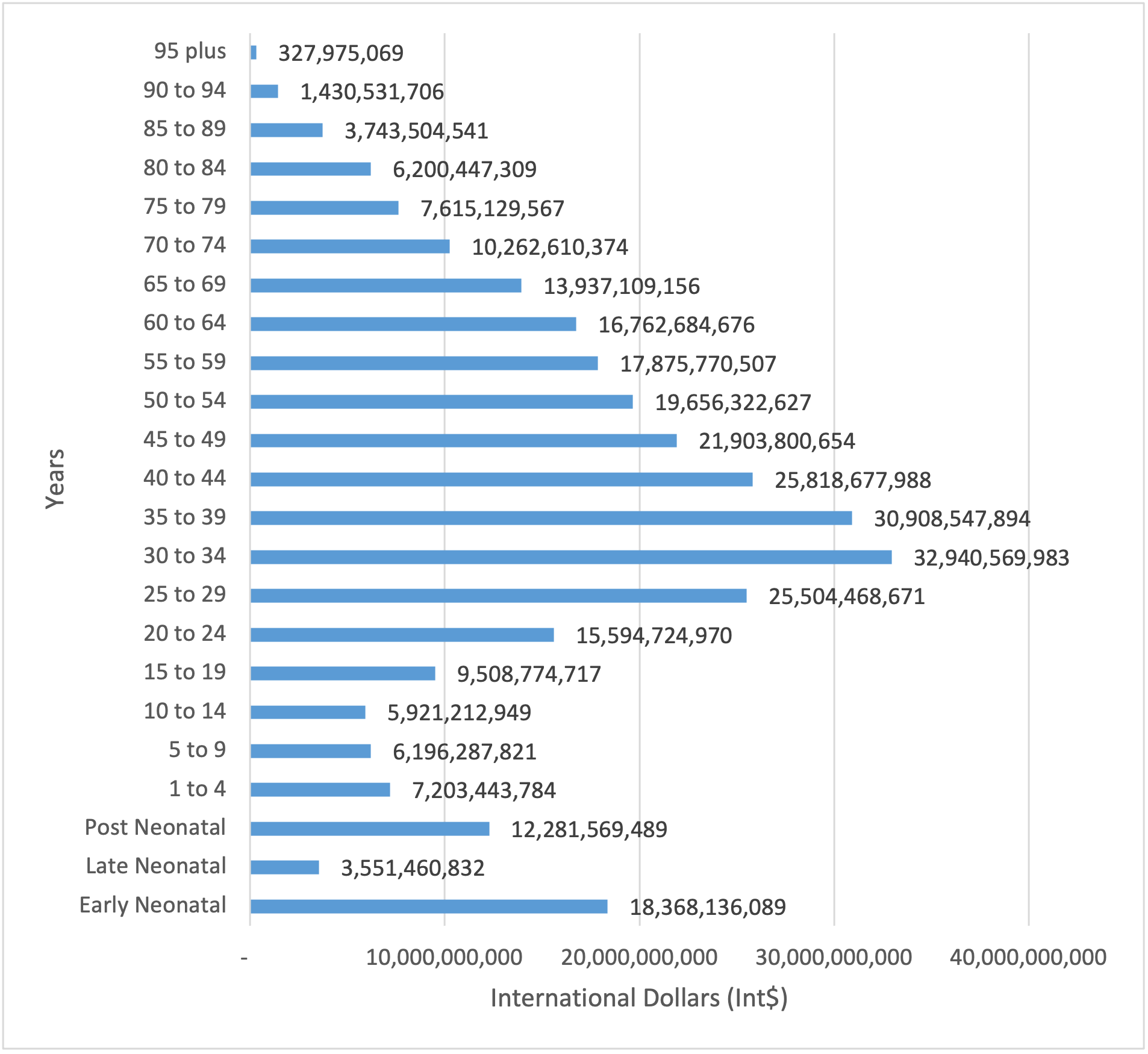
Figure 1 portrays the dollar value of DALYs from all causes by age groups. The South Africans aged 14 years and less sustained DALYs worth Int$ 53.5 billion (17%); the 15-59 year-olds incurred DALYs worth Int$ 199.7 billion (64%); 60-year-olds and above bore DALYs worth Int$ 60.3 billion (19%). Therefore, US$ 216.5 billion (69%) of the total dollar value of DALYs lost occurred among people aged between 15 years and 64 years, i.e. the most economically productive age bracket.
_from_all_causes_by_age_groups_i.png)
Communicable, maternal, neonatal, and nutritional diseases
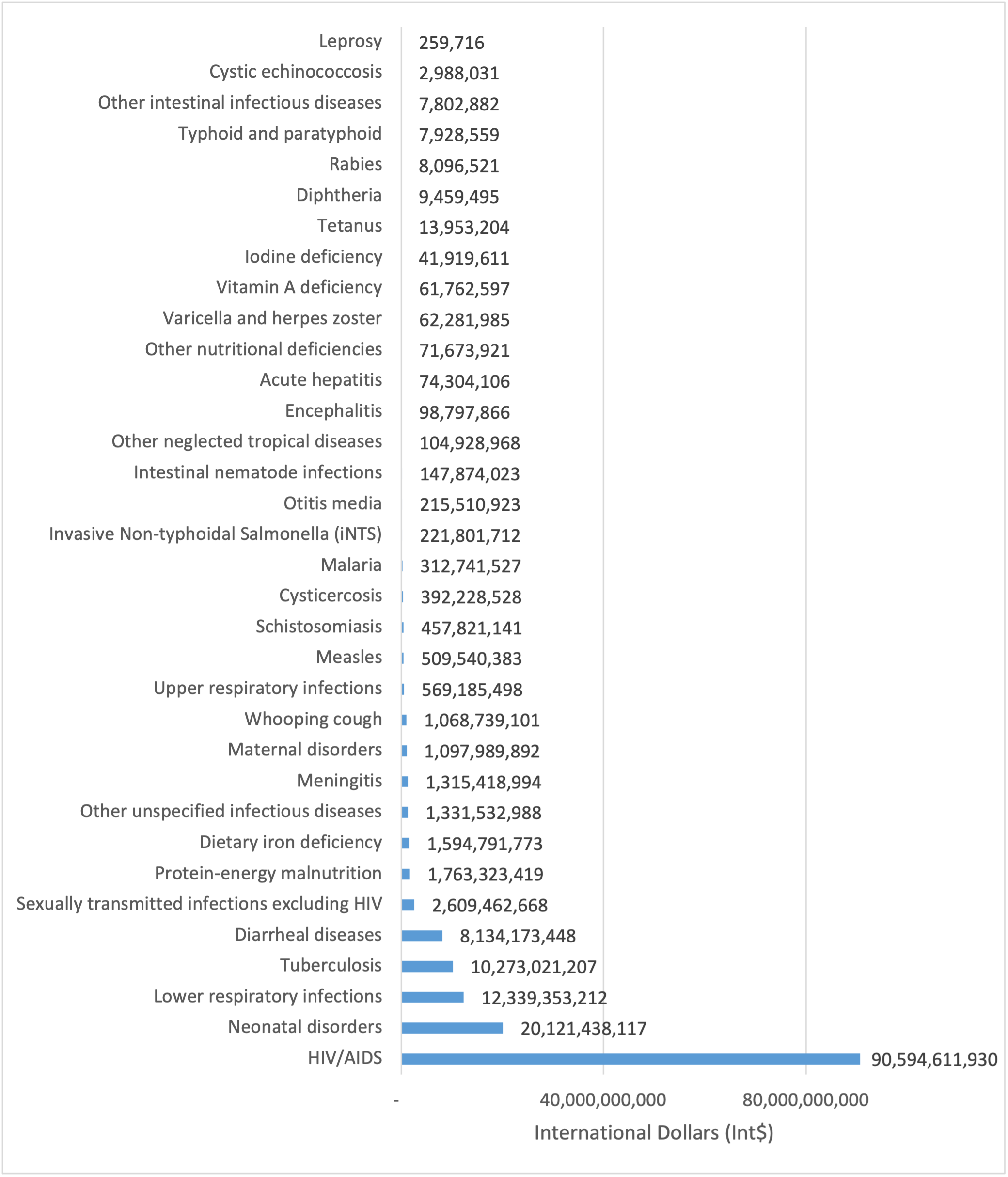
Figure 2 shows the dollar value of DALYs various CMNND categories. Of the total dollar value of DALYs from CMNND of Int$ 155.6 billion, 60% emanated from HIV/AIDS and sexually transmitted infections; 15% from respiratory infections and tuberculosis; 14% from maternal and neonatal disorders; 5% from enteric infections; 3% from other infectious diseases; 2% from nutritional deficiencies; and 1% from Neglected Tropical Diseases (NTD) and Malaria. Thus, about 91% of the total dollar value of DALYs was from five causes, i.e. HIV/AIDS, neonatal disorders, lower respiratory infections, tuberculosis, and diarrheal diseases.
_from_communicable__maternal__ne.png)
Noncommunicable diseases
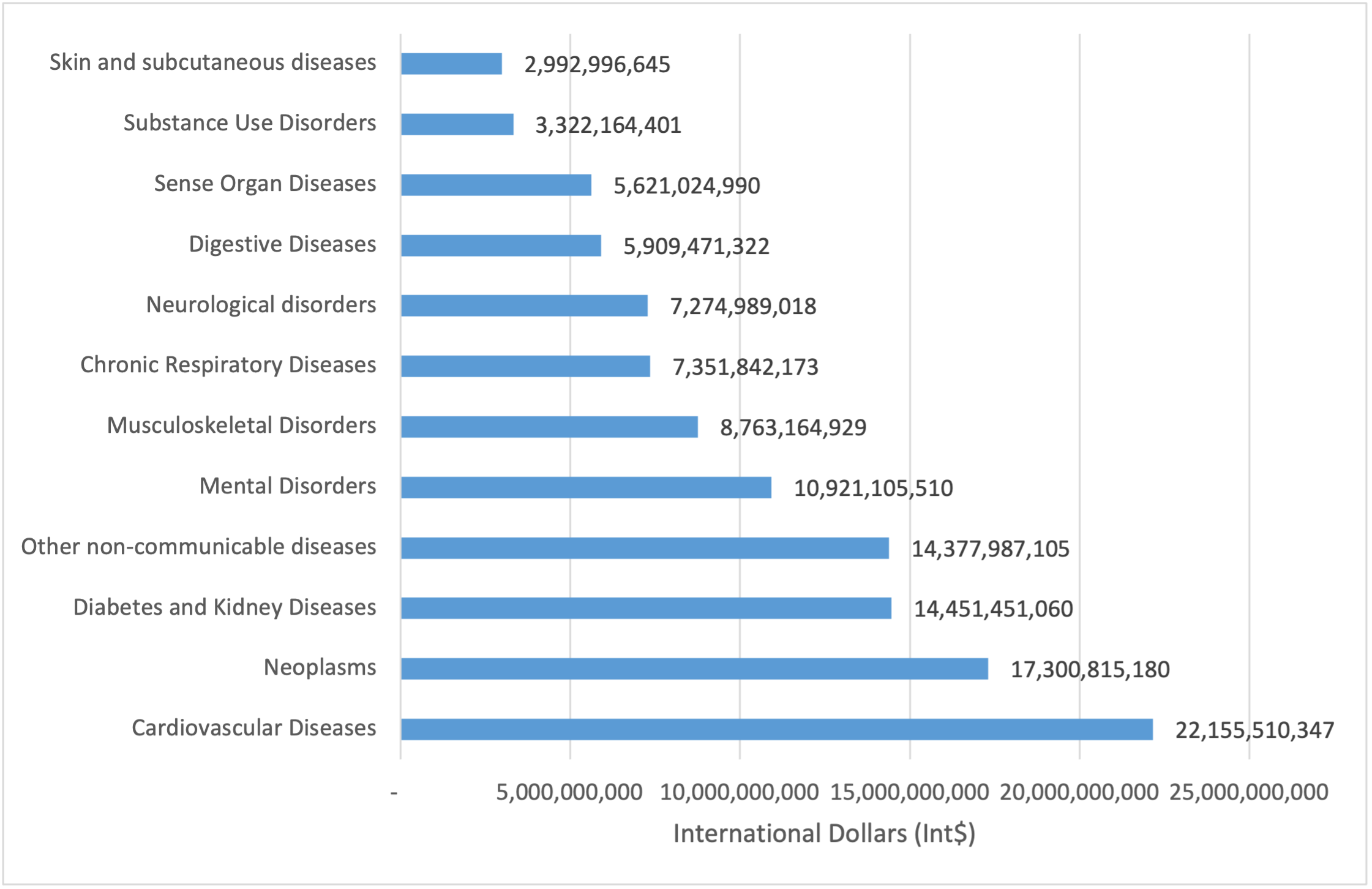
Figure 3 illustrates the dollar value of DALYs from the main categories of NCDs. Out of the total DALYs from NCDs valued at Int$ 120.4 billion, 18% was ascribed to cardiovascular diseases; 14% to neoplasms; 12% to diabetes and kidney diseases; 9.1% to mental disorders; 7.3% to musculoskeletal disorders; 6.1% to chronic respiratory diseases; 6.0% to neurological disorders; 5.0% to digestive diseases; 5.0% to sense organ diseases; 3% to substance use disorders; 2.5% to skin and subcutaneous diseases; and 12% to other non-communicable diseases (congenital birth defects, urinary diseases and male infertility, gynaecological diseases, haemoglobinopathies and haemolytic anaemias, oral disorders, and sudden infant death syndrome). On the other hand, diabetes mellitus, stroke, ischemic heart disease, depressive disorders, and chronic kidney disease made up 29% of the dollar value of DALYs from NCDs.
_from_noncommunicable_diseases_i.png)
Injuries
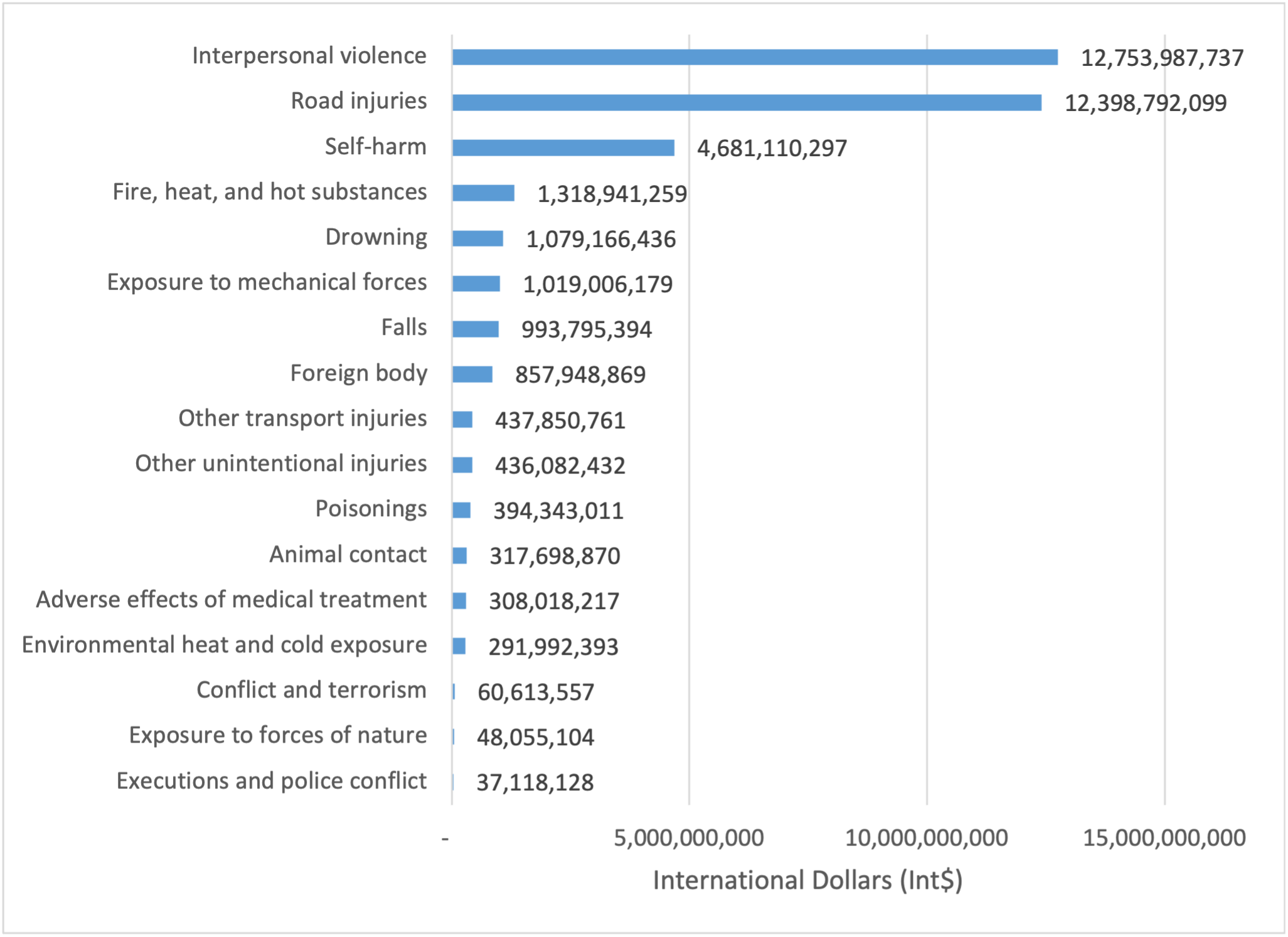
Figure 4 presents the dollar value of DALYs from all seventeen forms of injuries. Injuries caused DALYs worth a total of Int$ 37.4 billion. Self-harm and interpersonal violence accounted for Int$ 17.5 billion (47%), transport injuries for Int$ 12.8 billion (34%), and unintentional injuries for Int$ 7.1 billion (19%). Eighty-seven per cent of the total dollar value of DALYs from injuries was due to interpersonal violence (34%), road injuries (33%), self-harm (13%), drowning (3%), and fire, heat, and hot substances (4%).
_from_injuries_in_south_africa_(.png)
Dollar Value of DALYs in 2019 From Five SDG3-Related Targets
In 2019 SDG3-related diseases and health conditions resulted in a total of 21.7 million DALYs that had a dollar value of Int$ 256.4 billion (82%). As depicted in Table 2, 90% of the dollar value of SDG-related DALYs accrued to neonatal mortality, HIV/AIDS, and NCDs alone.
Forecast of Reductions in Dollar Value of DALY Losses in South Africa Assuming the Five SDG 3-Related Targets Are Accomplished by 2030
Table 3 portrays the dollar value of DALYs in 2019, the dollar value of DALYs in 2030, and predicted savings per SDG health condition/disease.
We forecast that attaining the five SDG3 targets would lead to approximately a 45% (Int$139.75 billion) drop in the total national dollar value of DALYs by 2030.
Discussion
Key findings
According to Institute for Health Metrics and Evaluation (IHME) Global Burden of Disease Collaborative Network database, the Republic of South Africa incurred a total of 26.6 million DALYs from all causes in 2019.3 Using net GDP per capita of Int$ 11,791.60 per DALY, the study reported in this paper valued the national stock of DALYs at Int$313.5 billion.
It would be wrong to assume that if all the causes of DALY loss were eradicated, South Africa would increase the total GDP of Int$313.5 billion. That is because 28.7% of South Africa’s total labour force was unemployed in 2019, and people aged below 15 years and above the compulsory retirement age of 64 are arguably not part of the labour force.1 When ratifying the International Labour Organization (ILO) Minimum Age Convention of 1973, South Africa specified the minimum employment age as 15 years.76
Critiques may argue that the DALYs lost among the population aged below 15 years and above the compulsory retirement age should be valued at zero. However, the total dollar value of DALYs lost among people aged between 15 and 64 years was Int$216.5 billion in 2019. Adjusting this estimate further by unemployment rate yields a value of Int$ 154 billion, i.e. 216.5 x ((100 - 28.7)/100)). That is equivalent to 20% of South Africa’s total GDP of US$ 761.8 billion in 2019. Therefore, it is clear that even with adjustment for both minimum working age and unemployment rate, disease burden exerts a significant burden on South Africa’s economy.
Implications for policy
SDG3.1 and SDG3.2: Maternal and Neonatal Disorders
South Africa could prevent loss of DALYs worth approximately Int$ 8.3 billion per year if SDG targets SDG3.1 and SDG3.2 are accomplished by 2030. In 2017 South Africa had a universal health coverage index for reproductive, maternal, newborn and child (RMNCH) health services of 79 (where the target is 100),77 signifying a gap of 21 points, which need bridging to have a chance of realising targets SDG3.1 and SDG3.2. According to the Department of Health, attainment of SDG3.1 and SDG3.2 will require universal coverage of maternal health services, vaccines against preventable diseases, and integrated management of childhood diseases services detailed in the national health sector strategic plan.66 Development of the RMNCH aspects of South Africa’s strategic plan 2020/21-2024/25 was informed by the WHO Regional Committee for Africa (RC) road map for accelerating the attainment of the MDGs related to maternal and newborn health in Africa78; the global strategy for women’s, children’s and adolescents’ health (2016-2030) (GSWCAH),79 and its operational framework.80 The development of South Africa’s strategic plan was also apprised by the WHO World Health Assembly (WHA) resolutions on GSWCAH81; maternal, infant and young child nutrition82,83; female genital mutilation84; global vaccine plan85,86; the role of the health system within a national multisector response to address interpersonal violence against women, girls and children87; global newborn health action plan88; global immunisation strategy89; United Nations Commission on Life-Saving Commodities for Women and Children recommendations90; and reduction of perinatal and neonatal mortality.91
Implementation of the interventions contained in the strategic plan for reducing maternal, child, infant, and neonatal mortalities is underpinned by section 27 of the South Africa Constitution that assures right of access to health care, food, water and social security92; the National Health Act of 200393; the Choice on Termination of Pregnancy Act of 199694; the National Health Insurance Bill.95
The South African Government efforts to curb maternal, child, infant, and neonatal mortality are buttressed by pertinent African Union declaration,96 and Charters on human and people’s rights on women’s rights in Africa,97 and the rights and welfare of the child.98
Furthermore, the Government’s actions to curb maternal, child and neonatal mortality are in line with recent United General Assembly Resolutions on the elimination of all forms of violence against women and girls99; elimination of female genital mutilation100; intensification of efforts to end obstetric fistula101; high-level political declarations on UHC102; rights of the child103; and preventable maternal mortality and morbidity and human rights.104
SDG3.3 Tuberculosis, HIV/AIDS, Malaria, Acute Hepatitis, and NTDs
The attainment of SDG target 3.3 would annually save South Africa DALYs worth approximately Int$ 75.3 billion from HIV/AIDS, Int $8.7 billion from tuberculosis, Int$ 835.6 million from NTDs, Int$ 281.5 million from malaria, and Int$ 48.3 million from acute hepatitis. In short, the country would salvage DALYs with a total value of Int$ 85.13 billion.
The UHCSCI component of these infectious diseases had a score of 62, denoting a shortfall of 38 in coverage of health services/interventions aimed at preventing and controlling HIV/AIDS, TB, NTDs, malaria, and acute hepatitis.77 Bridging the gap calls for full implementation of the infectious diseases strategies and actions outlined in the Department of Health Strategic Plan 2020/21-2024/25.66
The development of goals, targets, strategies, and actions aimed at combating infectious diseases was informed by the WHO World Health Assembly (WHA) resolutions on preventing and controlling HIV and viral hepatitis,105 TB,106 malaria,107 and vector-borne diseases.108,109
Pertinent African Union decisions/documents110–115 and the United Nations General Assembly Resolutions116–119 underpin South Africa’s efforts to implement strategies and actions to attain infectious diseases-related SDG3 target 3.3.
SDG3.4: NCDs
South Africa would salvage DALYs worth Int$40.15 billion should it succeed in attenuating the disease burden from NCDs by a third by 2030 (SDG target 3.4).65 The UHCSCI component of NCDs had a score of 58 (on a scale of 0-100),77 signifying a deficit of 42 points in coverage of health services/interventions targeted at addressing associated risk factors. Such a gap in coverage of essential health services ought to be bridged by implementing NCD strategies and actions in the Department of Health Strategic Plan 2020/21-2024/25.66 The development of goals, targets, strategies and actions geared at bridging NCD services gaps were informed by the WHO World Health Assembly (WHA) resolutions titled global action plan on physical activity 2018–2030120; global strategy on diet, physical activity and health121; global action plan for the prevention and control of NCD 2013–2020122; the global strategy for the prevention and control of NCD123; the comprehensive mental health action plan 2013–2020124; the WHO Framework Convention on Tobacco Control.125 The implementation of the NCD-related strategies and actions in the South Africa Department of Health Strategic Plan 2020/21-2024/25 is reinforced by the African Union Commitment AUC-WHO/COM.3/2014 on NCDs in Africa,126 and the United Nations General Assembly Resolutions A/RES/74/2,127 A/RES/66/2,128 and A/RES/74/244129 on prevention and control of NCDs, and resolution A/RES/74/244 on consuming fruits and vegetables.130
SDG 3.6: Road Injuries
South Africa to half the road injuries by 2030 (SDG target 3.6)65 would save DALYs worth Int$6.2 billion. The achievement of SDG target 3.6 depends on both performance of Road Traffic Management Corporation (TRMC), mandated by law to manage road traffic and enforce relevant laws, and the national health system provision of adequate coverage of pre-hospital and post-crash care services.
The TRMC was established in 2005 through the Road Traffic Management Corporation Act No. 20 of 1999.131 The TRMC is legally mandated “To provide, in the public interest, for co-operative and coordinated strategic planning, regulation, facilitation and law enforcement in respect of road traffic matters by the national, provincial and local spheres of government; to regulate the contracting out of road traffic services; to provide for the phasing in of private investment in road traffic; to provide for connected matters” (p.1).131 The aim of TRMC is “to promote safety, security, order, discipline and mobility on the roads, and to protect road infrastructure and the environment” (p. 1).131
The National Road Traffic Act governs law enforcement regarding road traffic matters No. 93 of 1996 and its amendments.132,133 The Act covers registration and licensing of motor vehicles, manufacturers, builders and importers; driver’s fitness testing and licensing; vehicle fitness testing and issuance of roadworthy certificate; operator fitness, registration and issuance of card; powers and functions of Director-General concerning road safety; appointment of dangerous goods inspector; road traffic signs and general speed limit; duties of drivers and garages concerning accidents and accident reports; and penalties for driving while under the influence of intoxicating liquor or drugs.132,133 The TRMC has a critical role in preventing and curbing the incidence and severity of road traffic accidents through rigorous assurance of quality roads, the fitness of vehicles, and enforcement of the road traffic Act.
An assessment of the TRMC ten key performance indicators (KPI) in the 2015-2020 strategy revealed that only four (40%) were achieved.134 That included: educating and creating awareness in road traffic matters, ensuring compliance with traffic legislation through effective and efficient enforcement, promoting the prevention of fraud and corruption in the road traffic fraternity, and creating a conducive environment by inculcating a culture of learning and high performance.134 The two KPI’s on establishing and sustaining relationships with interest groups on road traffic matters; and establishing an integrated national road traffic information system were partially achieved.134 Lastly, the four KPI’s on professionalising the road traffic fraternity, investing in road safety research and development, developing and monitoring norms and standards for the road traffic fraternity, and promoting and sourcing investment from the private sector for road safety were not achieved.134
The TRMC Strategic plan 2020/21 – 2024/2025 aims to achieve a 50% reduction in road fatalities from the 2018 base year and achieve a higher external and internal positive perception of the RTMC.134 The TRMC planned activities would need to be complemented with health system investment to bridge the existing health service coverage and access gap of 20 points (i.e. out of a target of 100).77 It is critically important to ensure that South Africa’s health system (at national, provincial and district levels) can safeguard road accident victims’ enjoyment of their constitutional right to emergency health services, including immediate post-accidence response, trauma care and rehabilitation services.
The development of the TRMC Strategic Plan was informed by the Brasilia Declaration on Road Safety135 and the World Health Assembly Resolutions WHA69.7136 and WHA57.10 on road safety.137 The African Union Road Safety Charter138 and the United Nations General Assembly Resolution A/RES/74/299 on improving global road safety139 provides high-level political support for implementing TRMC Strategic Plan and health system strengthening of pre-hospital, hospital, post-hospital and reintegration services for road traffic accident victims.
Limitations
This study has some limitations inherent in DALY estimations and HCA employed in the monetization of DALYs. First, this study suffers shortcomings inherent in 2019 DALY estimations. The limitations in estimations of population and fertility are explained by Vollset et al.,140 global diseases and injuries by GBD 2019 Diseases and Injuries Collaborators,141 risk factors,142 and demographics.143
Second, in his article entitled “Calculating the global burden of disease: time for a strategic reappraisal?” the late Professor Alan Williams argued that DALY estimates could not be used to monitor population health, to establish priorities between interventions, and to guide research priorities.144 He argues that the information needed in priority setting is incremental gains and incremental costs associated with alternative health interventions in specific public health problems.
Third, GDP has been criticized for not taking into account negative externalities of the economic production process (e.g. pollution),145 ignores distribution (or equity), ignores the contribution of housewives (full-time homemakers), and does not make people happier above a certain threshold of the higher material standard of living.146–149
Fourth, strictly applied, the human capital approach would value the DALYs accrued among children aged below 15 years, adults above retirement age (65 years and above), the unemployed, and persons who cannot work due to severe disablement at zero. That might consequently bias health development investments against these segments of society. Such discrimination would be going against South Africa’s Constitution that proclaims every citizen right of access to health services, sufficient food, water, and social security66; the WHO Constitution150; and the United Nations Universal Declaration of Human Rights (UDHR)151. Therefore, to avoid contravening the South African Constitution, the WHO Constitution and the UDHR, we decided to value all the DALYs accruing to all age groups at the same net GDP per capita.
Fifth, our study is based on the monetary valuation of the DALYs incurred by South Africa in 2019. It does not capture the health impact of the global Coronavirus Disease (COVID-19) pandemic, whose spread to South Africa was confirmed on 5 March 2020.152 By 24 July 2021, the country had conducted 14.5 million (equivalent to 24% of the population) COVID-19 tests that confirmed a total of 2.4 million cases, i.e. 2.2 million recovered cases, 144 thousand active cases, and 70 thousand deaths.153 Therefore, the monetary value of DALY estimates and forecasts reported in this paper may be an underestimation.
Conclusion
The DALYs sustained had an estimated dollar value equal to 41% of South Africa’s national GDP in 2019. Achievement of the SDG3 targets by 2030 would save the country DALYs worth Int$ 139.72 billion. In addition, adequate funding and implementation of existing health-related policies, legislations, strategies, and priority programmes plans might optimise national (including provincial and district) health system performance, and as a result, facilitate the bridging of extant gap in UHC service coverage index and subsequent attainment of SDG3 targets.
The evidence contained in this article can be used in two ways. First, inform the process of updating the expiring priority national programmatic strategic plans and advocacy for sufficient funding to tackle priority SDG-related health conditions. For example, the dollar value of DALYs could inform the revision of South Africa’s Strategic Plan for the Prevention and Control of Non-Communicable Diseases, which expired in 2017.154
Second, in advocacy with both the Government and private sector to increase annual investment into the national health system from US$526 (in 2018) to US$984 per person (with 60% from general government expenditure on health) as proposed by Stenberg et al. for the attainment of SDG3.19
The dollar value of DALY estimates is intended purely for use in advocacy for increased funding into health-related sectors in pursuit of national and international health development goals.65,66 There is an urgent need, where contextualized evidence does not exist, for economic evaluations of health promotion, disease prevention and control interventions to guide priority setting and decision-making in South Africa.
Acknowledgements
We owe profound gratitude to Jehovah Maccaddeshem for meeting all our needs in the entire process of writing this paper. The JoGHEP Editor and the two anonymous peer reviewers provided constructive suggestions that have been used to improve the quality of our paper. The views expressed are solely those of the authors and should not be attributed to their affiliated institutions.
Author Contributions
FS, CH, and JMK designed the study; reviewed relevant literature; assembled data from IMF, IHME and WHO databases; developed dollar valuation model in Excel Sheets; analysed data; interpreted results, and drafted the manuscript. All authors approved the final version of the paper.
Declaration of Conflicting Interests
The authors completed the ICMJE Unified Competing Interest form (available upon request from the corresponding author), and declare no conflicts of interest
Ethical Approval and Consent to Participate
The analysis relied entirely on the secondary data published freely accessible international databases of the IHME, IMF, and WHO. Thus, ethical approval was not required.
Funding
The authors did not receive any financial support for the research, authorship, and publication of this paper.
Availability of Data and Materials
The secondary data analysed in the course of this study is freely available from the following websites:
-
GDP data from International Monetary Fund (IMF) World Economic Outlook Database database1: https://www.imf.org/en/Publications/WEO/weo-database/2020/October
-
Current health expenditure per person data from World Health Organization (WHO) Global Health Expenditure Database18: http://apps.who.int/nha/database/Select/Indicators/en
-
DALY data from the Institute for Health Metrics and Evaluation (IHME) database3: http://ghdx.healthdata.org/gbd-results-tool
Correspondence
Joses Muthuri Kirigia, ASDRC
P.O. Box 6994 00100, Nairobi, Kenya
Email: muthurijoses68@gmail.com.
Tel: +254 720 664 167.