Understanding any research field often begins with a generalized search, where some of the first questions are often related to research publication output. Our fascination with this metric stems from the “publish or perish paradigm”,1 regardless on the downsides of this approach.2,3 This kind of analysis enables not only broad insight, but can further describe trends useful in critical analysis of the research field.4,5
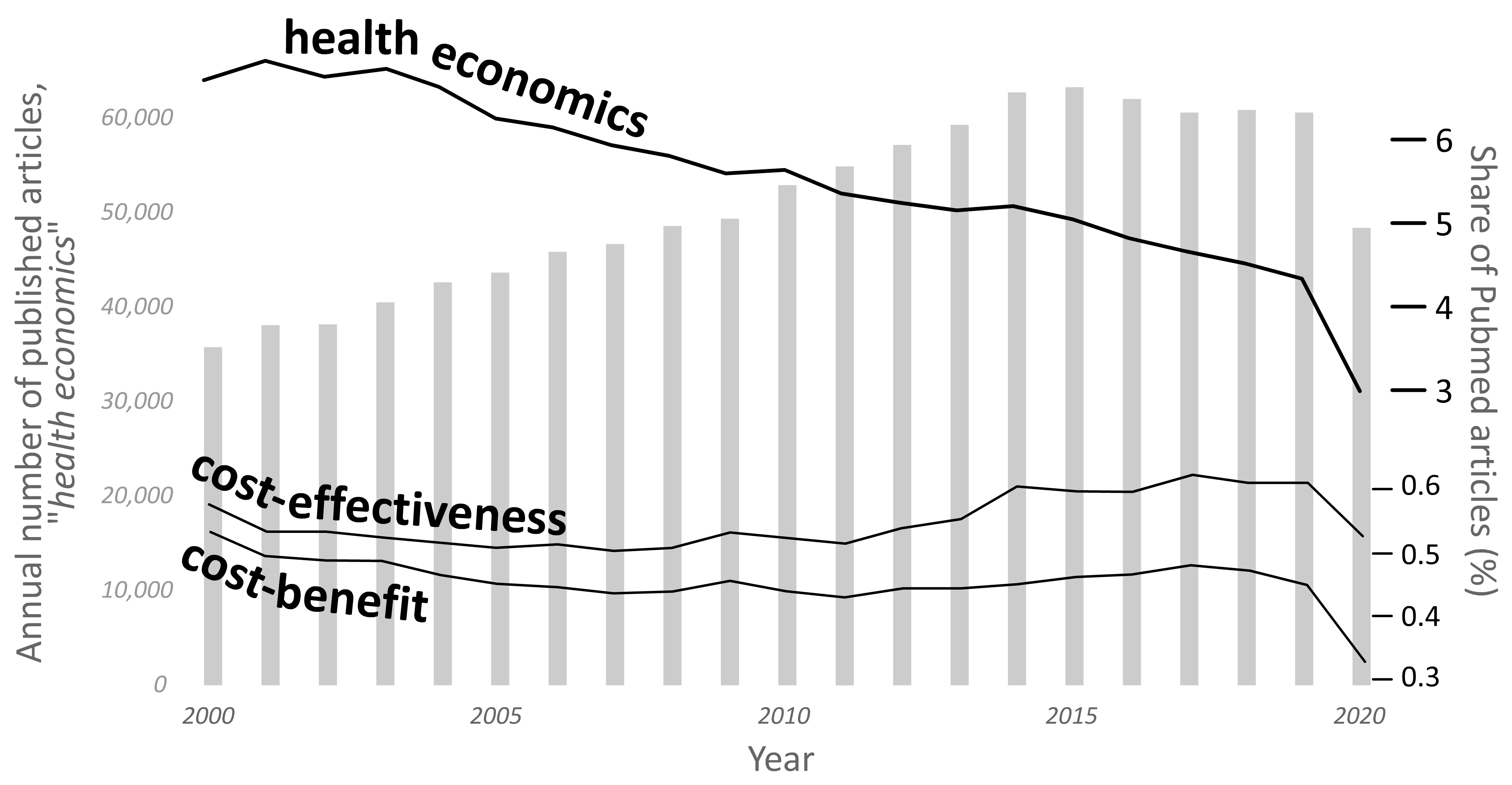
Previous analysis of the field of health economics reported very favourable patterns, and suggested likely pathways of development, published in the January of 2016.6 However, the situation seems to have changed. During 2000-2020 there were just over a million articles indexed by PubMed (https://pubmed.ncbi.nlm.nih.gov/), which had utilized “health economics” as a keyword (search performed May 14, 2021). Breakdown according to year suggested an average value of over 50,000 articles annually, with the greatest number of all articles published in 2015 (Figure 1, grey bars; Table 1, published). Interestingly, the number of published articles seems to have declined afterwards, never again surpassing the peak in 2015. The situation becomes even clearer when these number are adjusted to the total number of articles indexed by PubMed, which was constantly rising, suggesting that the share of articles related to health economics was on a steady decline (Figure 1, black line). While health economics was mentioned in close to 7% of all articles in 2000, this percentage had declined to only 3% in 2020. Although one might argue that 2020 is indeed a special case due to the COVID-19 pandemic, the decline is clearly seen even in the years preceding this. Actually, if we consider the years 2000-2015 as the referent ones, it is possible to calculate the projected number of articles in a linear projection model. Such a model has an R2 of 0.99, and suggests that the predicted number of published articles during 2016-2020 should be slightly over 333 thousand articles, while only 291 thousand articles were published during this period. This means that the field of health economics had a net loss of over 42 thousand articles, just during these five years (Table 1, column predicted). The year 2020 is even more worrying, since by adding another keyword, COVID seems to deal an additional blow to the filed; the removal of the COVID related articles from the 2020 count (by excluding the papers that also had this keyword), suggested the additional loss of 7600 articles, suggesting that the number of published articles that were not dealing with COVID had declined from slightly over 60 thousand in 2019 to 40 thousand in 2020, or a decline of 32%.

A more in-depth analysis with the two most common study types: the cost-effectiveness and the cost-benefit analysis, suggests minor deviations from the constant share (Figure 1, lower black lines). At the very least, it seems that the methodologically more demanding types of studies retained their constant share in the total number of published articles on PubMed, without an indication of the decline that was obvious for the entire field of health economics.
Although methodologically somewhat unreliable, the addition of the region as yet another keyword suggested that the number of articles related to Europe and America were on a decline, while those related to Asia, Africa and Australia were substantially rising (Table 1).
What could be the reason for this stagnation and decline? Does this mean that we measured it all? Is there nothing more to evaluate? Hardly. If ever, we need health economics now, in the time of global pandemic crises, to assist and aid in decision-making process. What more, we need to substantially expand outreach to health economic studies, the use of evidence-based methods and aim for the best possible evidence. These tasks are very demanding, as they have roots in the improvements of the data collection process, health care organization and health systems, which are all almost daunting tasks on their own. This will become especially important in the post-COVID era,7–9 which will require substantial improvements in the way health care is being organized and managed, globally.
Funding
None received.
Author contributions
OP is the sole author.
Competing interests
OP is the Editor-in-Chief of the Journal of Global Health Economics and Policy. To ensure that any possible conflict of interest relevant to the journal has been addressed, this article was reviewed according to best practice guidelines of international editorial organizations. The author has completed the ICMJE Unified Competing Interest form (available upon request from the author) and declares no conflicts of interest.