Immunisation is one of the most effective public health interventions, significantly reducing morbidity and mortality from vaccine-preventable diseases. Globally, immunisation programs have played a pivotal role in controlling, eliminating, or eradicating diseases such as polio, measles, and smallpox.1,2 Although vaccines are highly effective, the success of immunisation programs and overall health outcomes depend on the quality of service delivery.3–7
Ethiopia has made substantial progress in expanding its immunisation coverage over the past decades, with the government prioritising the expansion of primary healthcare services.8–11 However, while national immunisation coverage rates have improved, the quality of immunisation services remains a critical area of concern.8,12 Quality in immunisation can be assessed through two main dimensions: technical quality, which refers to the competence of service providers in delivering vaccines safely and effectively, and perceived quality, which reflects mothers’ and caregivers’ satisfaction and trust in the service. Both aspects are essential for ensuring high immunisation coverage and effectiveness.13–15
In Ethiopia, challenges such as inadequate infrastructure, workforce shortages, competency/skill gaps and logistical barriers often impact the technical quality of immunisation services.8 Moreover, cultural beliefs, misinformation, and communication gaps between vaccinators and clients can influence the perceived quality of these services.16 However, the quality of the immunisation session and the client’s perception of the immunisation service were not explicitly documented in Ethiopia. Assessing the technical and perceived quality of the immunisation service can provide comprehensive insight into the strengths and weaknesses in current immunisation quality, offering actionable insights for improving service delivery.
This study aims to evaluate the quality of immunisation services in Ethiopia through the dual lenses of technical and perceived quality, encompassing pre-, intra-, and post-administration immunisation practices, as well as the satisfaction of mothers and caregivers. By understanding the current status of service quality, we can identify critical areas for improvement, enhance vaccine delivery, and ultimately contribute to achieving higher immunisation coverage and better health outcomes in the country.
METHODS
Survey design
This study was part of a national immunisation program evaluation survey aimed at assessing various components of the immunisation program, including session quality and mothers/caregivers’ satisfaction. The evaluation encompassed both the technical competency of vaccinators, assessed through direct observation during vaccination sessions, and caregiver satisfaction, gauged via exit interviews with mothers and caregivers.
Study setting and period
The study included all regions and city administrations of the country, except the Tigray region, due to the conflict. The Expanded Program on Immunisation (EPI) is provided at all regions and city administrations, at Health centres, health posts, and hospitals, including some private health facilities. The study was conducted from March to July 2023.
Study population
Vaccinators were the study population for assessing the quality of immunisation sessions through direct observation. In addition, mothers/caregivers who came for child vaccination services formed the study population for assessing their satisfaction.
Sample size and sampling
The sample size for the study was calculated based on the health facilities across regions and city administrations in the country. The determined sample sizes complied with the minimum guidelines set by the WHO for cluster surveys.17 A two-stage stratified sampling method was employed to choose the health facilities. In the first stage, enumeration areas (EAs) were randomly selected from stratified sampling frames that categorised urban and rural EAs, which were prepared for each region and city administration by the Ethiopian Statistical Services (ESS).
In each region, both urban and rural enumeration areas (EAs) were represented according to their population sizes, with 21.4% of EAs from urban settings and 78.6% from rural areas. Health facilities situated within the selected EAs and those nearby were included in the study. Overall, there was a proportional distribution of health facilities, comprising 291 health posts, 316 health centres, and 76 hospitals across various EAs, regions, and city administrations. Each health facility hosted between three and five vaccination sessions. Using a combination of expert judgments and Guidelines for Implementing Supportive Supervision18 Recommendation three to five session observations (2971) and exit interviews (2955) per facility were conducted to ensure valuable insights about the vaccinators’ competency and mothers/caregivers’ satisfaction, respectively.
Data collection tools and procedures
A vaccination session observation checklist was used to assess the competency of vaccinators in delivering immunisation services. The checklist included key activity indicators designed to evaluate vaccinator practices across three stages: pre, intra, and post-administration. A total of 21, 19, and 2 activity indicators were used to assess the pre-administration, intra-administration, and post-administration practices of vaccinators, respectively. Data collectors (observers) were recruited based on their previous experience with immunisation programs. Having experience in immunisation supervision and having completed the Immunisation Trainer of Training (ToT) training, these individuals were used to recruit the data collectors. A total of 115 data collectors participated in the data collection process. Although we used trained and experienced session observers, we didn’t conduct an inter-rater reliability assessment. Additionally, five Likert scale questions (10) were developed based on literature reviews7,19,20 to assess the satisfaction of mothers and caregivers with immunisation services. These questions addressed various aspects, including waiting time, cleanliness of the session, waiting area conditions, opening hours, availability of vaccinators, respect shown by vaccinators, and the information provided by vaccinators to mothers/caregivers. The data was collected using the Open Data Kit (ODK) Collect toolbox to reduce data entry errors and obtain real-time data.
Measure of immunisation service quality
The quality of immunisation services was assessed through both technical and perceived quality measures. Technical quality was evaluated by observing vaccination sessions, with a focus on the competency and adherence of vaccinators to key immunisation practices. Vaccinators’ performance was assessed using selected indicators that covered pre-, intra-, and post-administration activities during the vaccination sessions. Additionally, the perceived quality of the immunisation service was assessed through exit interviews with mothers/caregivers who attended the child immunisation service, which collectively evaluated their satisfaction with the vaccination service.
Data analysis
The vaccination session observation practice percentage was computed and interpreted separately for each indicator. We calculated the performance percentage of vaccinators based on activity indicators for pre, intra, and post-administration practices. Additionally, the level of satisfaction of mothers/caregivers was assessed by computing the score for each of the five Likert scale questions independently. We then created an index by categorising “very satisfied” and “satisfied” responses as “satisfied”, while the remaining responses (very dissatisfied, dissatisfied, and neutral) were classified as “dissatisfied”.
RESULTS
Session observation and mothers/caregivers’ exit interview characteristics
A total of 2,971 session observations were conducted, with the majority (75.6%) from rural settings. The majority of session observations were conducted at the health centres (63.6%), followed by health posts (19.2%). In addition, 24.1% of the sessions were observed from the Oromia region, followed by Amhara (23.8%) (Table 1).
A total of 2,955 mothers/caregivers were interviewed, 24.9% were from Oromia and 21.8% were from Amhara regions. The majority (77.3%) were under 30 years of age, with 64.4% being homemakers. Regarding religion, 44.2% were Muslim, followed by Orthodox (34.2%) and Protestant (20.4%). Most respondents lived in rural areas (62.8%) and were married (98.1%). Additionally, 64.8% had families larger than four members (Table 2).
Pre-administration vaccination safety practice
Only four per cent of vaccinators conduct a complete and proper infant assessment before vaccination. In addition, only 11% of the vaccinators used different education materials for immunisation-related communication. The practice of delivering key messages about immunisation was also practised by only 7% of the vaccinators. Almost half the vaccination sessions were delivered by a single vaccinator. Additionally, the proper reconstitution of BCG and measles vaccines was performed by 58% and 66% of the vaccinators, respectively (Table 3).
Intra-administration vaccination safety practice
The observation also showed that 9% and 11% of the vaccinators missed the correct route and site during BCG administration, respectively. In addition, 8% and 9% of the vaccinators missed the correct route and site during Measles administration, respectively. Seven percent of the vaccinators also didn’t provide the correct dose of the Rota vaccine. The finding also showed that seven percent of the vaccinators didn’t administer Penta and PCV vaccines with the correct route and site (Table 4).
Post-administration vaccination safety practice
Eighty-five percent and 80% of the vaccinators avoid needle recapping and properly use the safety box, respectively (Table 5).
Maternal/caregiver satisfaction with the vaccination service
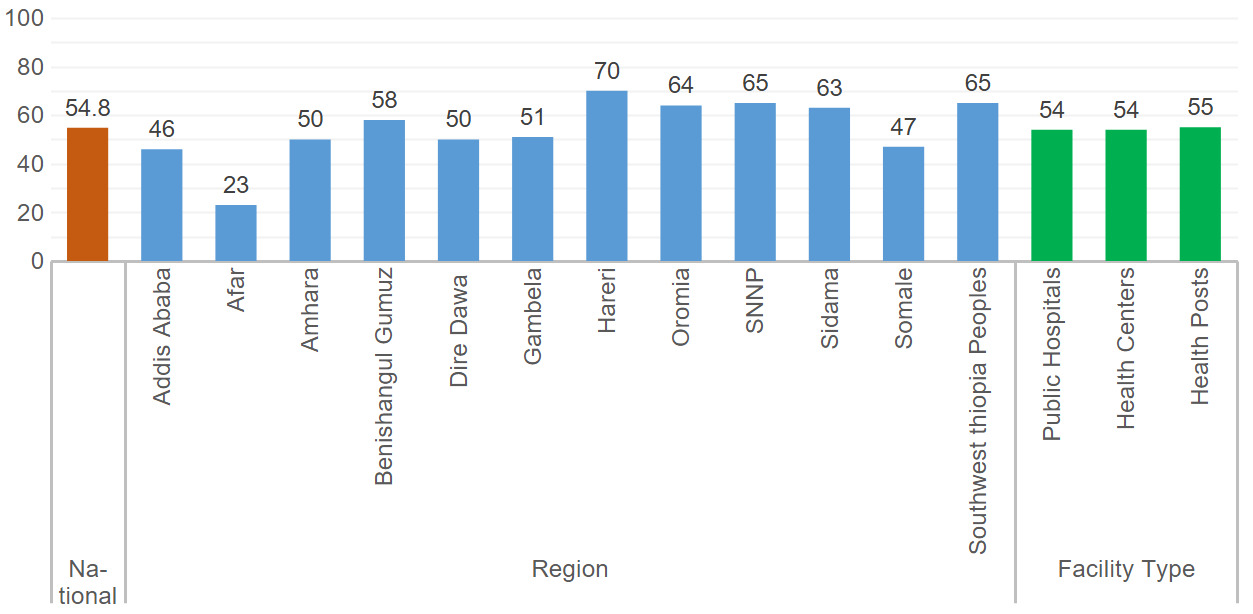
The study showed that only 55% of the mothers/caregivers reported being satisfied with the vaccination service. Satisfaction varied across regions, ranging from 23% (Afar) to 70% (Harari) (Figure 1).

DISCUSSION
This study reveals sub-optimal immunisation session quality and client dissatisfaction with the immunisation service delivery. Only 4% of vaccinators conducted a complete infant assessment before vaccination, and just 11% used educational materials for effective communication. Moreover, only 7% of vaccinators delivered key immunisation messages, and nearly half of the sessions were handled by a single vaccinator. Alarmingly, 9% and 11% of vaccinators failed to follow the correct route and site for BCG administration, while 8% and 9% did the same for measles. Additionally, 7% administered incorrect doses of the Rota vaccine, and similar errors in route and site were found with Penta and PCV vaccines. Eighty-five per cent of vaccinators avoided needle recapping, and 80% used safety boxes correctly. The findings highlight gaps in the quality of immunisation sessions, with low adherence to assessment, communication, and vaccine administration protocols. The study also noted that 55% of mothers/caregivers reported satisfaction with the service.
In this study, the practice of complete infant assessment is low, indicating a significant gap in ensuring the readiness of infants for vaccination. Hence, a thorough assessment is crucial for identifying potential contraindications or health conditions that could affect the safety of vaccines.21 Almost one in ten vaccinators used educational materials for communication, reflecting a missed opportunity to enhance caregiver understanding, trust, and engagement in the vaccination process. Without adequate communication, caregivers may not fully grasp the importance of vaccines or know how to manage post-vaccination care.22 Moreover, the delivery of key immunisation messages practised by less than one in ten of vaccinators indicates a serious communication gap. Poor sharing of key immunisation messages with mothers/caregivers may contribute to vaccine hesitancy, as caregivers are not fully informed about the antigens and related information.23 Additionally, with almost half of the vaccination sessions handled by a single vaccinator, this resulted in a reduction in service quality due to time constraints, high workloads, and a lack of attention to both clinical and communication practices.
In this finding, almost one in ten vaccinators didn’t adhere to the correct route and/or site for BCG and Measles vaccine administration. Improper administration can compromise the effectiveness of the vaccines and increase the risk of adverse reactions. Additionally, about one in ten of the vaccinators commit errors in correctly administer Penta and PCV vaccines with the right route and/or site, which affects the vaccines’ protection against multiple diseases, and improper administration may leave children vulnerable to infections.12 Approximately one in ten vaccinators administered the incorrect dose of the Rota vaccine, potentially compromising its efficacy and reducing the ability to achieve the desired immune response in infants.24 These findings are aligned with different studies done in Ethiopia, which also showed gaps in immunisation service quality.12 The identified intra-administration gaps might result from several factors, including the absence of standardised immunisation quality guidelines, insufficient training, high patient volumes, and workloads. Addressing these issues is essential to ensure the safety and effectiveness of vaccination service delivery.
Almost four in five of the vaccinators avoided needle recapping and properly used safety boxes. However, the remaining 20% vaccinators failed to avoid needle recapping and didn’t use safety boxes correctly, which represents a significant safety concern. Needle recapping is a well-documented cause of accidental needle stick injuries, and improper disposal of used syringes can expose healthcare workers, waste handlers, and the community to infectious materials.8,25
Another key finding was the low satisfaction of mothers/caregivers with vaccination services, with only half of the mothers/caregiver’s expressing satisfaction. This indicates that nearly half of mothers/caregivers were dissatisfied with immunisation services. This can erode trust in the immunisation service, leading to vaccine hesitancy and higher dropout rates.26 Poor immunisation service experiences, coupled with ineffective communication and misinformation, may further discourage caregivers from completing the immunisation schedule. When key immunisation messages are not properly conveyed, caregivers may misunderstand vaccine benefits, increasing susceptibility to misinformation and negative perceptions, ultimately reducing vaccine uptake and coverage. This implies that it’s crucial to improve service quality, enhance communication strategies, and ensure the accurate dissemination of information to boost vaccine uptake and coverage. This necessitates a comprehensive review of service quality, with a focus on reducing waiting times, enhancing facility cleanliness, and improving the overall experience for mothers and caregivers.7,19,27 Addressing these issues could not only improve satisfaction rates but also contribute to higher vaccination coverage and public confidence in immunisation programs.
CONCLUSIONS
The study highlights considerable challenges to the quality of immunisation services in Ethiopia. Only a few vaccinators undergo a complete and thorough infant assessment before administering vaccines, and a small portion of vaccinators utilise educational materials to support communication with caregivers. The practice of effectively delivering essential immunisation messages was also notably low among vaccinators. Moreover, there were issues with proper vaccine administration, particularly in ensuring that vaccines such as BCG, measles, Rota, Penta, and PCV were administered using the correct route, site, and dosage. In terms of post-administration safety practices, a relatively high proportion of vaccinators adhered to avoiding needle recapping and using safety boxes correctly. However, the overall client satisfaction with vaccination services remained low. These findings suggest a need to establish an immunisation service quality standard, fostering a culture of accountability, and comprehensive improvements in the training and supervision of vaccinators, with a focus on enhancing both technical skills and communication abilities. Moreover, improving communication between vaccinators and caregivers, particularly through the use of educational materials and clear messaging, is crucial to boosting trust and satisfaction in immunisation services. Such actions will enhance communication effectiveness and overall service quality, ultimately improving the experiences and health outcomes of mothers and caregivers.
ACKNOWLEDGEMENTS
We extend our appreciation to the CBMP consortium universities for their academic and technical support. We are grateful to Amref Health Africa for funding the study and to WHO, UNICEF, JSI, and PATH for providing vital logistical assistance. We also acknowledge the Ministry of Health, as well as all regional, zonal, and woreda health offices, health facilities, and health posts, for their cooperation in facilitating field activities. We would like to extend our sincere gratitude to the participating communities, caregivers, and health workers for their time and invaluable contributions to this research.
DISCLAIMER
The views expressed in this article are solely those of the authors and do not necessarily represent the official positions of the Ministry of Health or partner organisations.
ETHICS STATEMENT
Ethical approval for this study was obtained from the Institutional Review Board of Hawassa University (IRB/288/15). Additional support letters were obtained from the Ministry of Health and the Regional Health Bureaus. Written informed consent was obtained from all participating mothers/caregivers and vaccinators. Data were collected using an anonymous electronic data collection system to ensure confidentiality and privacy.
DATA AVAILABILITY
The data supporting the findings of this study are available from the authors upon reasonable request. The dataset is not publicly available due to institutional data-sharing policies.
FUNDING
This study received financial and logistical support from Amref Health Africa, UNICEF, WHO, JSI, and PATH. The funders had no role in the design of the study, data collection, analysis, interpretation of the results, manuscript preparation, or the decision to publish.
AUTHORSHIP CONTRIBUTIONS
GA, BFE, YA, BD, LD, AT, AA, MA, KG, GT, SS, BT, and KA conceptualised and designed the study, conducted data analysis, prepared the first draft of the manuscript, supervised data collection, validated the findings, and critically revised and edited the manuscript. MM, NW, MN, YL, MZ, and MA contributed to study conceptualisation, conducted formal data analysis, supported data curation and resource coordination, reviewed and edited the manuscript, and supervised data collection. All authors reviewed and approved the final manuscript.
DISCLOSURE OF INTEREST
The authors completed the ICMJE Disclosure of Interest Form (available upon request from the corresponding author) and disclose no relevant interests.
ABBREVIATIONS
AEFI – Adverse Events Following Immunisation
BCG – Bacille Calmette–Guérin
CI – Confidence Interval
EAs – Enumeration Areas
EPI – Expanded Program on Immunisation
ESS – Ethiopian Statistical Services
IRB – Institutional Review Board
LMICs – Low- and Middle-Income Countries
MoH – Ministry of Health
ODK – Open Data Kit
OPV – Oral Polio Vaccine
PCV – Pneumococcal Conjugate Vaccine
SD – Standard Deviation
SNNP – Southern Nations, Nationalities and Peoples Region
ToT – Training of Trainers
WHO – World Health Organisation