Vaccination is a proven and cost-effective strategy to reduce the high burden of child or population morbidity and mortality.1 Sustainable Development Goal (SDG) 3 envisions ensuring universal access to immunisation services.2 By 2030, the goal is to achieve at least 90% coverage for basic immunisations, ensuring more widespread protection against vaccine-preventable diseases.3 However, the 2023 World Health Organisation (WHO) report showed that only 6.5 million children are partially vaccinated, and 14.5 million did not receive the initial dose of the pentavalent vaccinations.4 The body of evidence reported low coverage for Human Papillomavirus (HPV) vaccination with overt geographic disparities, which ranged from 11 to 94%.5 Most of the adolescent girls in sub-Saharan Africa were not receiving HPV vaccination.6 Few small-scale Ethiopian studies reported low coverage of HPV vaccines. In Ethiopia, only about two-fifths of adolescent girls received HPV.7 Limited local reports revealed the poor coverage of COVID-19 vaccines.8,9
The Ethiopian National Expanded Program on Immunisation (EPI) was launched with six antigens (BCG, DPT, Measles, and OPV) in 1980 and has made notable progress in increasing the number of antigens between 2011 and 2020 (including HepB-Hib, PCV, Rota, Td, HPV, and COVID-19 vaccines) and currently reached thirteen for life course immunisation.10 The country has made notable strides in increasing access to immunisation services in the last two decades. Between 2000 and 2019, the coverage of Penta3 increased from 21.1% to 61%, and the proportion of children fully immunised increased from 14.2% to 43%.11,12 Ethiopia has also achieved tremendous results in reducing deaths among children over the last two decades, including a 52% decline in under-5 mortality from 123 deaths per 1,000 live births in 2005 to 59 deaths per 1,000 live births in 2019. Over the same period, infant mortality declined from 77 to 47 deaths per 1,000 live births.13,14
EPI made a significant contribution to the observed remarkable improvements in child survival. The country aims to achieve SDG-3, further reducing under-five deaths to less than 25 per 1,000 live births15 and attaining the global targets for all basic child immunisations, HPV, and COVID-19 vaccines, i.e., greater than 90%.16 Despite this, the vaccination uptake in the life course remains low, and outbreaks of VPDs continue to be observed in various Ethiopian regions.17,18 The health system, including the immunisation program, has faced challenges due to the COVID-19 pandemic and internal conflicts since 2019. However, comprehensive and nationwide assessments have not been conducted to fully understand the context of immunisation services. Regular monitoring of immunisation service uptake is essential to evaluate Ethiopia’s progress towards the SDGs and other national targets, and to identify areas that require special effort. However, none of the previous studies reported on the national life course immunisation coverage, i.e., from infancy to adulthood. There was limited evidence showing the uptake of national COVID-19 immunisation services. Therefore, this study assessed the coverage of immunisation services in the life course in all Ethiopian regions.
METHODS
Study setting, period and design
This is part of the national immunisation program evaluation survey conducted in all Ethiopian regions and city administrations, except Tigray, due to internal conflict, which posed a challenge to conducting fieldwork. The five Capacity Building and Mentorship Partnership (CBMP) universities, including Addis Ababa, Jimma, Haramaya, Hawassa, and Gondar, designed and evaluated the program. In addition, the Immunisation Interagency Coordinating Committee (ICC), the National Immunisation Technical Advisory Group (NITAG), and the Immunisation Technical Working Group (TWG) were involved in the study process. The study was conducted from March to July 2023
Population, sample size and sampling
This study included all children aged 12-35 months, women of reproductive age (15–49 years), adolescent girls (15–18 years), and individuals aged 12 years or older to estimate Child vaccination, Tetanus-Toxoid, HPV, and COVID-19 vaccine coverage, respectively.
The sample size was computed based on the WHO cluster survey guideline19 And considered the 2019 Ethiopian Demographic and Health Survey (EDHS) coverage reports for Pentavalent-3 (61.9%), zero dose (19.9%), and MCV2 (9.1%). We also assumed a 95% level of confidence, a 2% margin of error, a design effect of 3, a 10% nonresponse rate, and an expected number of eligible children for each administrative region of 482. This resulted in a minimum sample size of 15,158 households with children aged 12 to 35 months. The sample size for HPV (75%) and COVID-19 (35.5%) was also estimated, considering the expected coverage for the respective antigens. We obtained the minimum sample size of 6,900 for adolescent girls and 14,825 for adults.
The household survey included 11 regions and the two city administrations. A two-stage stratified cluster sampling technique was employed to select participants. Enumeration areas (EAs) that formed a cluster were randomly selected, with stratification by urban-rural status. Sampling frames were prepared for each region and city administrations by the Ethiopian Statistical Services (ESS). The number of EAs required per region and city administration was determined based on the size within the stratum (study regions) and proportion of the Ethiopian population living in urban and rural areas (21.4% urban and 78.6% rural). A total of 468 EAs (100 EAs from urban and 368 EAs from rural areas) were randomly selected for the survey.
The field teams delineated the sampled EAs using digital maps obtained from ESS. Each team prepared sampling frames of households with at least one target population, i.e., children, women, adolescent girls, and adult household members. On average, one EA comprised about 200 households, and we randomly (using a computer-generated random number) selected 30 eligible households per EA. When a household had more than one eligible member for the given target population, one was selected using a lottery. If the selected person was unavailable during data collection time, the data collectors revisited the household at least twice.
Data collection
A pre-tested, structured household survey questionnaire was used to assess the coverage of immunisation services among children, adolescents, women, and individuals aged 12 years or above. The questionnaire was adapted from the Ethiopian EPI guideline.,20 WHO and UNICEF.21 The English version questionnaire was translated into five local languages: Amharic, Afan Oromo, Afar, Sidama, and Somali.
Data collectors were recruited based on their fieldwork experience and fluency in writing and speaking the local languages of the survey area. A total of 466 field workers were involved, of whom 234 and 115 were recruited as household and health facility data collectors (having a minimum of a BSc degree in health science), respectively, and 117 were supervisors (having a minimum of an MPH or MSc degree). One field or local guide was assigned for every five EAs.
Outcome measures
The child immunisation status was assessed for children born within three years before the survey. Data collectors first checked the child’s vaccination history and asked respondents to present the vaccination card. If available, the card’s information, including antigens and vaccination dates, was recorded. If the mother reported vaccination but could not provide the card, health facility records were reviewed. As a last resort, caregivers’ recall was used. To minimise recall bias, interviewers asked about the injection site, administration route (e.g., oral or injection), and the vaccination schedule.
Child immunisation coverage, excluding MCV2, was calculated among children aged 12 to 23 months, while MCV2 coverage was estimated in children aged 23 to 35 months. Full immunisation coverage was defined as the proportion of children aged 12 to 23 months who received one dose of BCG, three doses of pentavalent vaccine, three doses of PCV, four doses of OPV, two doses of Rotavirus Vaccine, and one dose of measles vaccine. Children aged 12 to 23 months who did not receive the first dose of the pentavalent vaccine were defined as zero-dose children.22 The dropout rate for the pentavalent vaccine was calculated as the coverage difference between the first and third doses, divided by the coverage of the first dose, and then expressed as a percentage by multiplying by 100. The dropout rate for MCV1 was estimated as the difference between the coverage of the first dose of pentavalent vaccine and MCV1, divided by the coverage of the first dose of pentavalent vaccine, and then expressed as a percentage by multiplying by 100.
Data Quality
The Open Data Kit (ODK) system, equipped with logical controls, was used to collect data in five local languages. Data collectors and supervisors with prior experience in immunisation services were recruited. A seven-day training session was conducted for the field team on the study’s aim, ethics, data collection tools, interview procedures, and techniques. The questionnaires were pretested outside the study area, which has similar characteristics to the study settings. The central data management team regularly checked whether the data collection was conducted in the right household using GPS coordinates. Daily virtual discussions were held among the field and central teams to discuss the completeness of the data, coding challenges, and data collection issues, as well as potential solutions for action. Data was exported from the field to the central ODK server on a daily basis.
Data analysis
Descriptive statistics, including frequency, percentage, mean, and standard deviation, were used to describe participants’ characteristics and immunisation coverage. Graphs and tables were used to present the study findings. All analyses were adjusted for sampling weight. The sampling weight was calculated as the inverse of the probability of cluster and household selection. The coverage is further stratified by region, setting, and type of health facility.
RESULTS
Study characteristics
A total of 13,666 mothers or caregivers of children aged 12-35 months were interviewed, which yielded a response rate of 96.5%. Approximately half of the mothers or caregivers had no formal education, and two-thirds were homemakers or agricultural workers. The majority of caregivers received ANC follow-up (82%) for the index child and gave birth at a health facility (70%). In the study, 43.5% of the children were aged 12 to 23 months (Table 1).
For HPV vaccination coverage, 5,338 adolescent girls aged 15–18 were surveyed nationwide. Among the adolescent girls, 85% were attending formal education, and 80% had completed primary education. Additionally, over three-fourths of the participants were currently enrolled in school. Ninety-five per cent of the participants reported living with their caregivers or parents (Table 2).
Participants for the COVID-19 vaccination were assessed from 13,843 adults aged 12 years and above. The majority (88.7%) of the participants were married and living in an agrarian setting (60%). Besides, about half of the respondents had no formal education (Table 3).
Child immunisation coverage
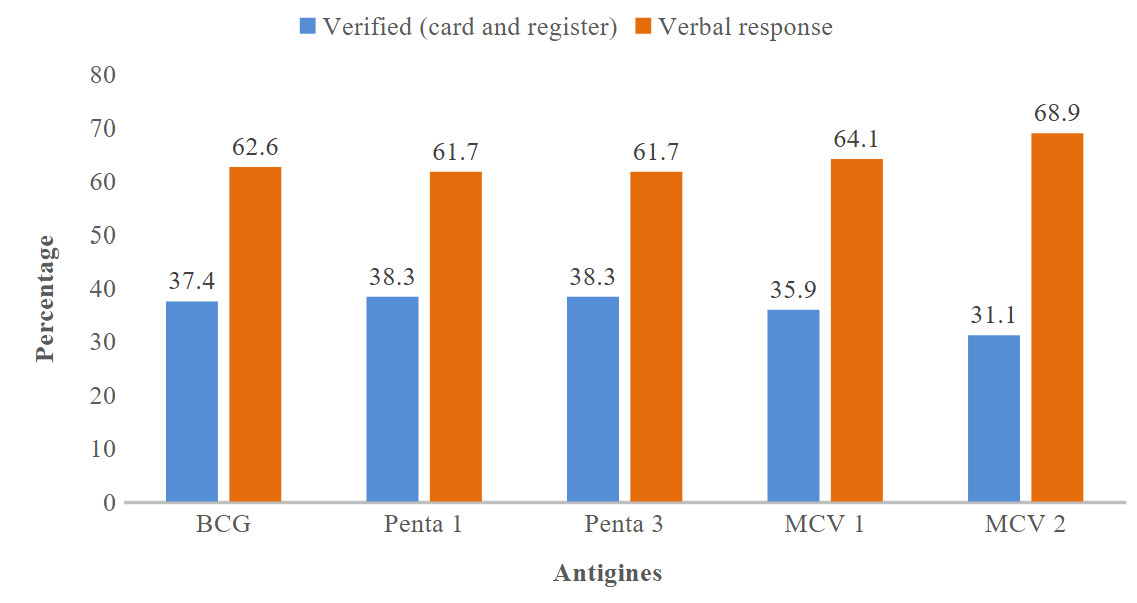
Assessment of vaccination card availability revealed that only 39.5% of respondents had a vaccination card. Among those without a card, 32.9% reported that the healthcare facility did not provide a vaccination card, 59.9% of them reported the card was lost, and 7.3% mentioned it had been torn or damaged. Vaccination status was verified through document checks (such as immunisation cards or registration records) or verbal confirmations from mothers and caregivers. The reported coverage for vaccine antigens, based on verbal responses, ranges from 61.7% to 68.9%, while the confirmed vaccine uptake, based on documentation, varies from 31.1% to 37.4% (Figure 1).

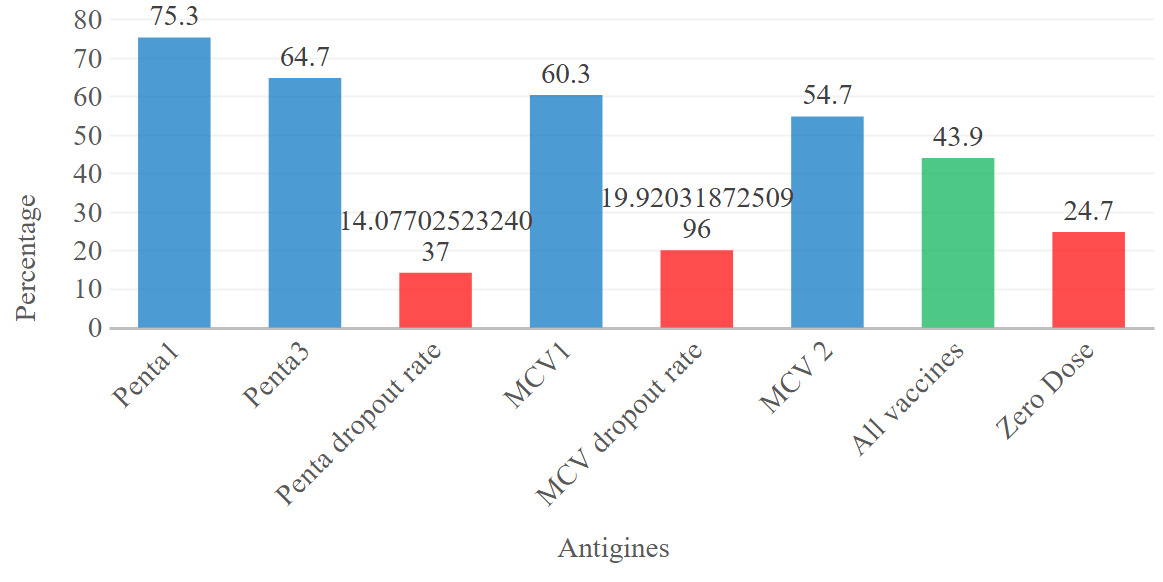
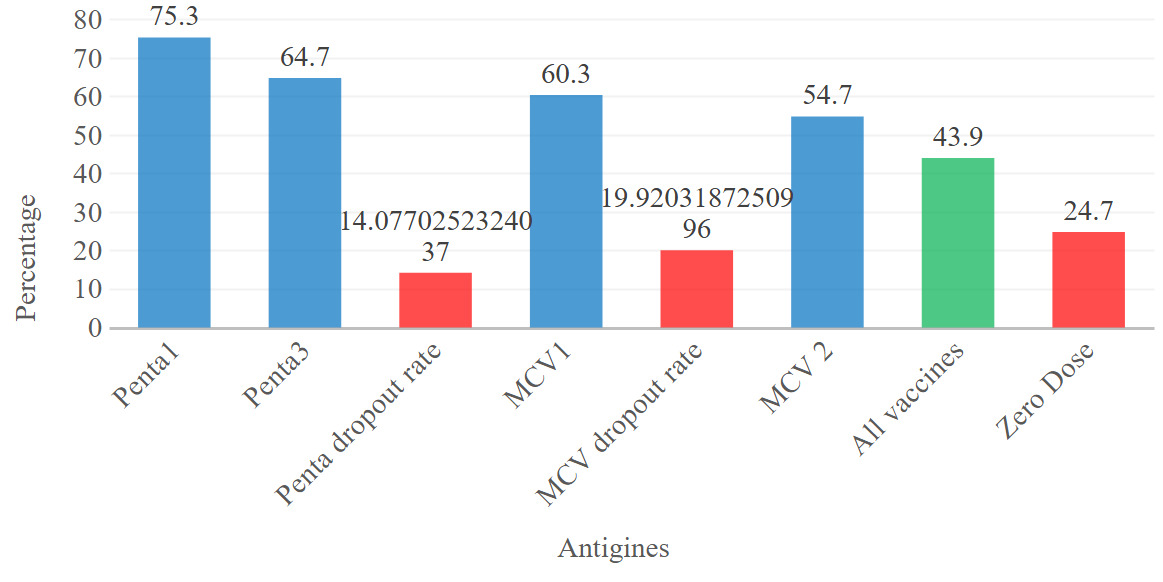
Two-thirds of children, 75.3% (74.2, 76.3), received the first dose of the pentavalent vaccine, and 64.7% (63.1, 65.7) took the third dose. About one in four children did not receive any scheduled vaccines. 60.3% (59.1, 61.5) and 54.7% (53.7, 55.8) received the first and second doses of MCV vaccines, respectively. Overall, only 43.9% (42.6, 45.1) of children complete the full schedule of vaccinations or receive all basic immunisations. The percentage of zero-dose patients was 24.7% (23.7%, 25.8%) (Figure 2).
Variation in child immunisation coverage
The findings reveal significant disparities in vaccination coverage across regions, residence types, education levels, and healthcare access in Ethiopia. Addis Ababa stands out with the highest full immunisation coverage at 74.3% and the lowest zero-dose rate at 1.0%. In contrast, the Afar and Somali regions report the lowest immunisation coverage, at 12.3% and 45.9%, respectively, with alarmingly high zero-dose rates of 40.0% in Afar and 40.7% in Somali. Oromia and Amhara also struggle, with substantial zero-dose rates of 27.7% and 24.2%, respectively. Urban areas have better full vaccination coverage at 51.2% and a low zero-dose rate of 11.1%, while pastoralist communities struggle with 29.0% coverage and a high zero-dose rate of 48.6%. Education has a significant influence on coverage, with mothers who have a college education achieving 54.0% coverage and a zero-dose rate of 4.0%. In comparison, those with no education have lower coverage (35.9%) and a higher zero-dose rate (33.4%). Antenatal care (ANC) attendance also plays a crucial role; mothers who attend ANC have 59.0% coverage, compared to 14.5% for those who do not. Children born in health facilities also have better coverage (61.8%) compared to those born at home (23.6%) (Table 4).
Td vaccination coverage
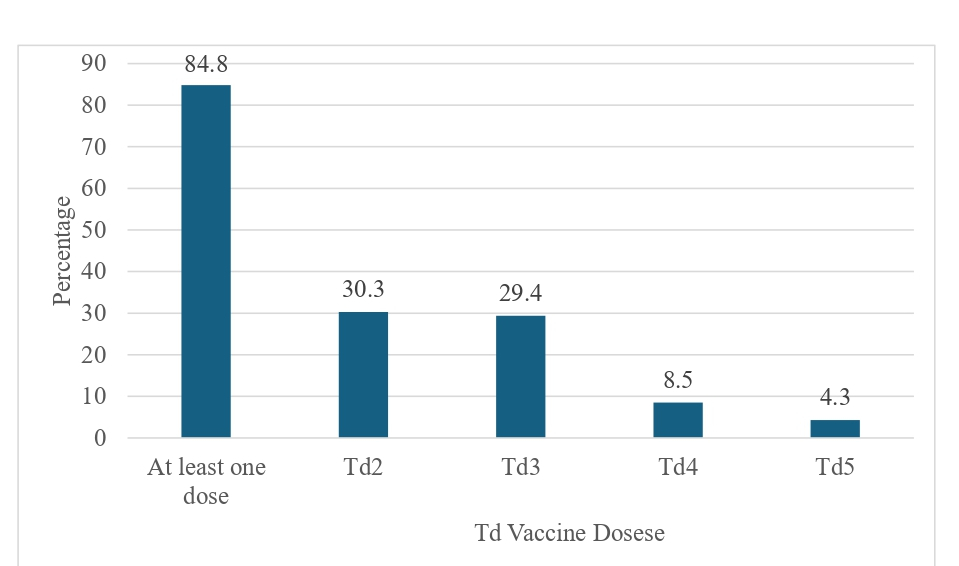
Most mothers (84.8%) received at least one dose of Tetanus-Diphtheria (TD) vaccination. Approximately one-third of mothers reported receiving the second and third doses, while very few (8.5% and 4.3%, respectively) received the fourth and fifth doses (Figure 3).

Variation of Td vaccination coverage
84.8% of mothers were exposed to at least one Td dose. Addis Ababa had the highest Td2 coverage (76.7%), while Somali had the lowest overall Td exposure (47.7%). College-educated mothers showed the highest Td exposure (93.1%) compared to those with no education (78.6%). Urban mothers had higher Td exposure (90.6%) than agrarian (84.2%) and pastoralist (70.5%) settings. Married mothers living together had an exposure rate of 84.9%, while those not living together had an exposure rate of 87.4%. Protestant mothers had the highest Td exposure (89.2%), compared to Muslim (81.7%) and Orthodox (85.2%) (Table 5).
HPV and COVID-19 immunisation coverage
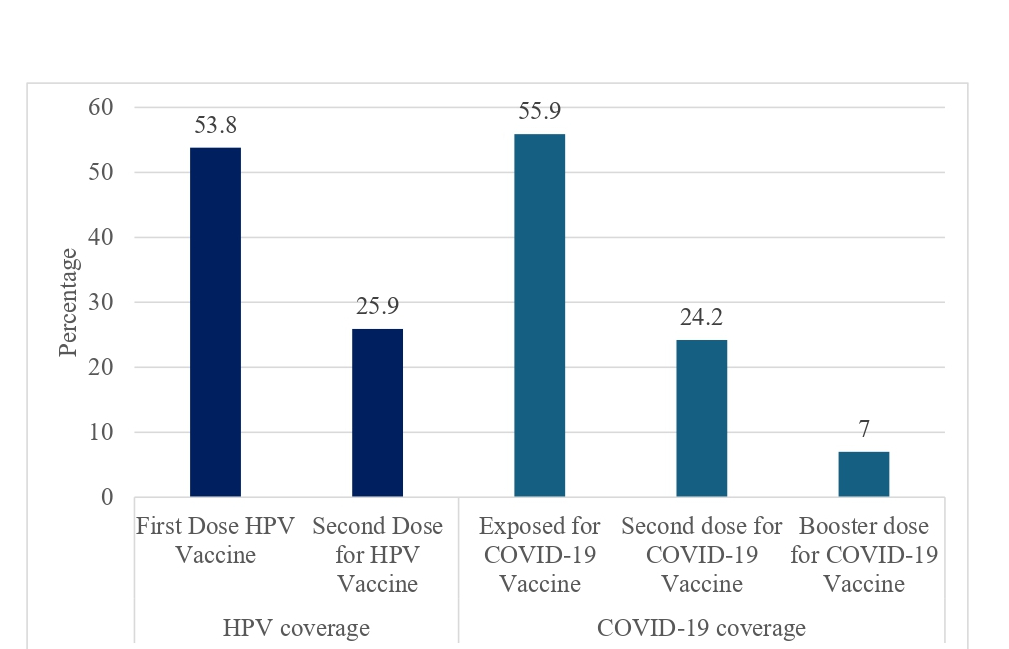
The coverage of the first (53.8%, 95% CI: 52.6-55.3) and second doses of HPV among adolescent girls was 53.8% (95% CI: 52.6-55.3) and 25.9%, respectively. About half (52.2%, 95% CI: 50.9-51.8) received the first dose of COVID-19, while 23.2% and 9.1% received second and booster doses of COVID-19, respectively (Figure 4).

Benishangul Gumuz had the highest HPV vaccination coverage (73.6%), while Somali had the lowest (32.8%). Girls aged 15 had the highest exposure (60%), while those aged 18 had the lowest (48.7%). Girls who can read and write had significantly higher vaccination rates (60.6%) compared to those who cannot read and write (15%). Urban areas (55.1%) had higher vaccination rates than pastoralist settings (36.5%). Protestant girls showed the highest two-dose rate (35.8%). Higher wealth quintiles correlated with increased HPV vaccination rates, peaking at 65.5% in the highest quintile.
DISCUSSION
This is the first national study to assess life-course immunisation coverage across various population groups. The findings revealed that two in five children were fully vaccinated, while one in four received no vaccines (zero-dose). Approximately 60% of individuals received the first dose of MCV1, with a 20% dropout rate, and nearly two-thirds received three doses of the pentavalent vaccine, with a 14% dropout rate. For maternal Td vaccination, five out of six women received the first dose, but only 4% completed the fifth dose. Only half of adolescent girls and adults were vaccinated for one dose of HPV and COVID-19, respectively.
The result showed that only two-fifths of young children aged 12-23 months received all basic immunisations, which falls significantly short of the national target of 90% by 2030 and the global averages. It was also far below the average coverage reported for sub-Saharan Africa or low- and middle-income countries.23 The low coverage for all basic immunisation was also reported by the 2019 Ethiopia Demographic and Health Survey (DHS) and the Performance Monitoring for Action panel.11 This low coverage puts two-thirds of Ethiopian children at a heightened risk of vaccine-preventable diseases (VPDs) and related mortality. The findings highlight the need for intensified efforts to improve immunisation access and delivery.
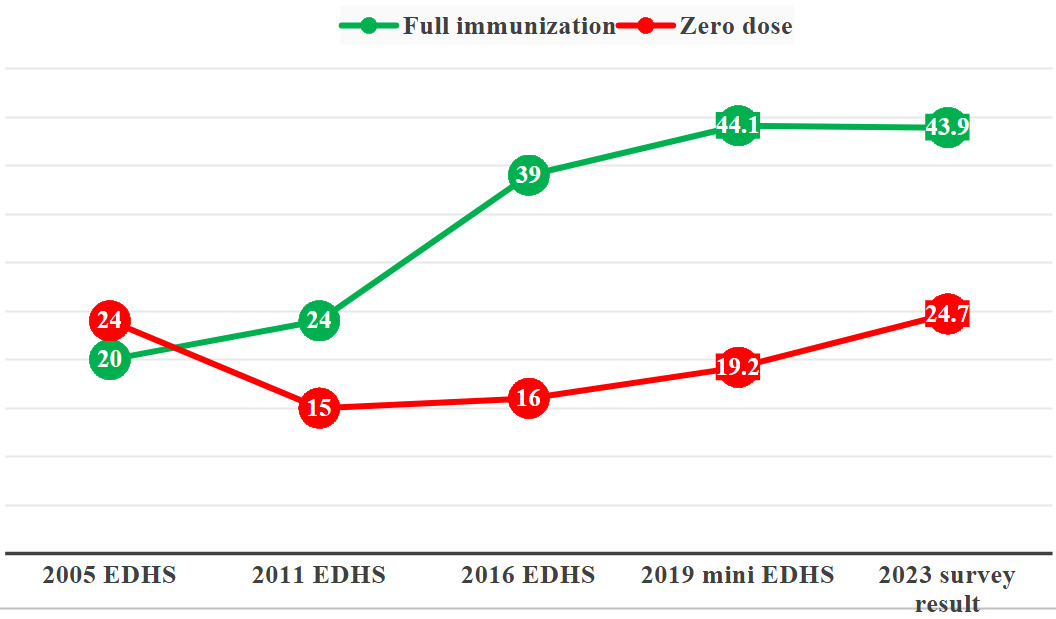
The 2023 survey reports a full immunisation rate of 43.9%, showing a significant increase from 20% in 2005 and 39% in 2016. This upward trend reflects improvements in the healthcare system, increased awareness, and effective immunisation campaigns over the years. The peak of 44.1% in 2019 indicates that the improvements in immunisation coverage may have plateaued since then, suggesting the need for renewed efforts to sustain and enhance these rates. The zero-dose immunisation rate has fluctuated over the years, decreasing from 24% in 2005 to 15% in 2011, but it rose again to 16% in 2019 and reached 24.7% in 2023 (Figure 5). This indicates a troubling trend where efforts to reduce the zero-dose population may have stalled or reversed recently. The rise in zero-dose rates since 2019 raises accessibility concerns, possibly due to factors such as the impact of the COVID-19 pandemic and conflicts in different parts of the country, which may have disrupted routine immunisation services and outreach efforts. The stagnation or increase in zero-dose rates suggests that specific barriers may not have been adequately addressed, particularly in underserved regions. The increase in full immunisation suggests that health policies and interventions have had a positive impact. However, the corresponding rise in zero-dose rates highlights gaps that need to be filled to ensure that improvements are equitable and reach the most vulnerable populations.

The findings reveal significant disparities in vaccination coverage across regions in Ethiopia. While Addis Ababa benefits from high immunisation rates and low zero-dose populations, regions such as Afar, Somali, Oromia, and Amhara experience much lower coverage and a higher prevalence of zero-dose children. Ongoing conflicts in Amhara and Oromia may affect vaccine access and uptake, particularly through campaigns and outreach approaches, due to travel restrictions. Furthermore, the nomadic lifestyle in pastoralist areas would affect the establishment of permanent vaccination sites, thereby limiting both access to and uptake of services.
These disparities highlight deep-rooted inequalities in healthcare access, particularly in rural and underserved communities. Addressing these challenges requires targeted interventions, such as enhancing healthcare infrastructure, implementing mobile vaccination units, and increasing community engagement through education campaigns.
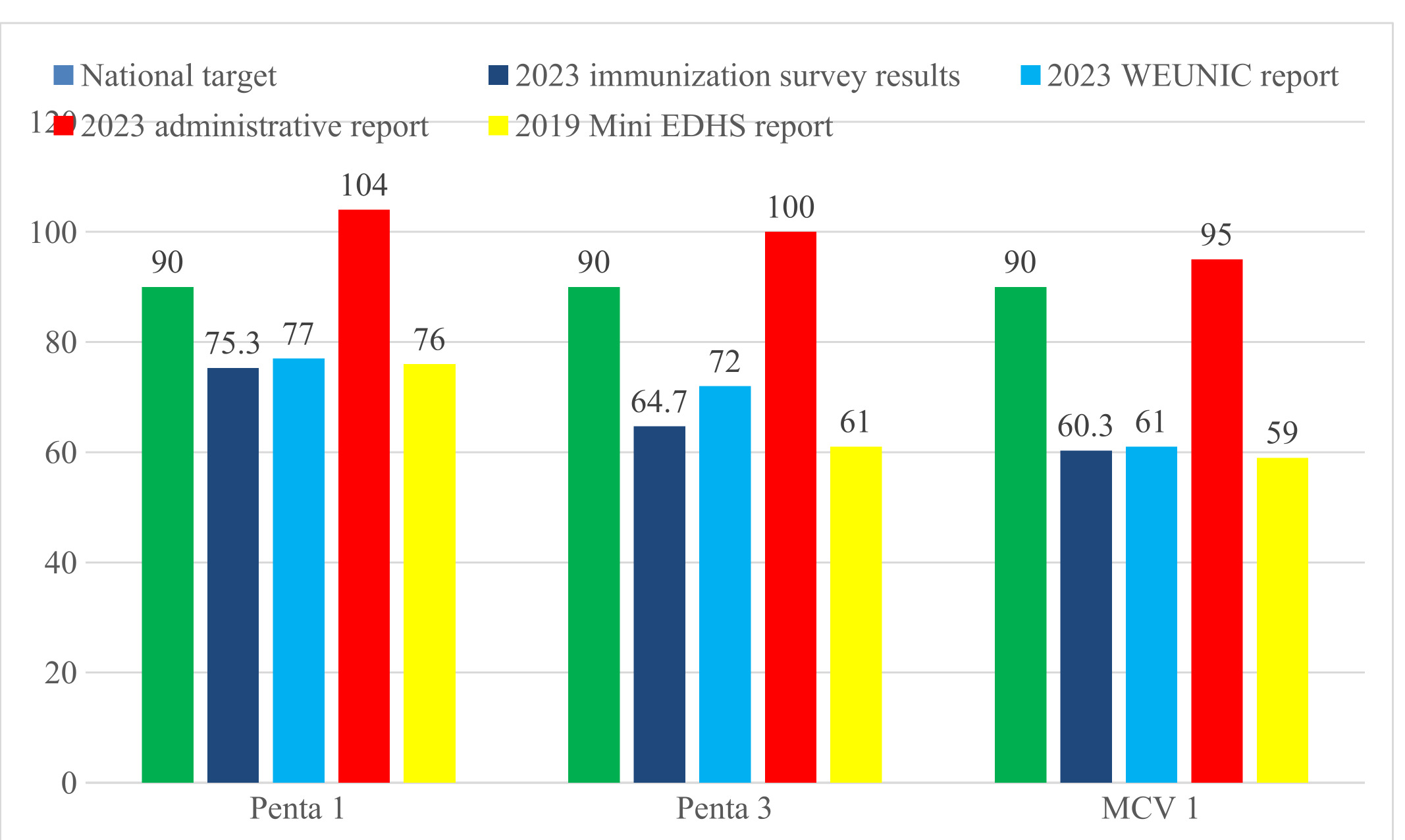
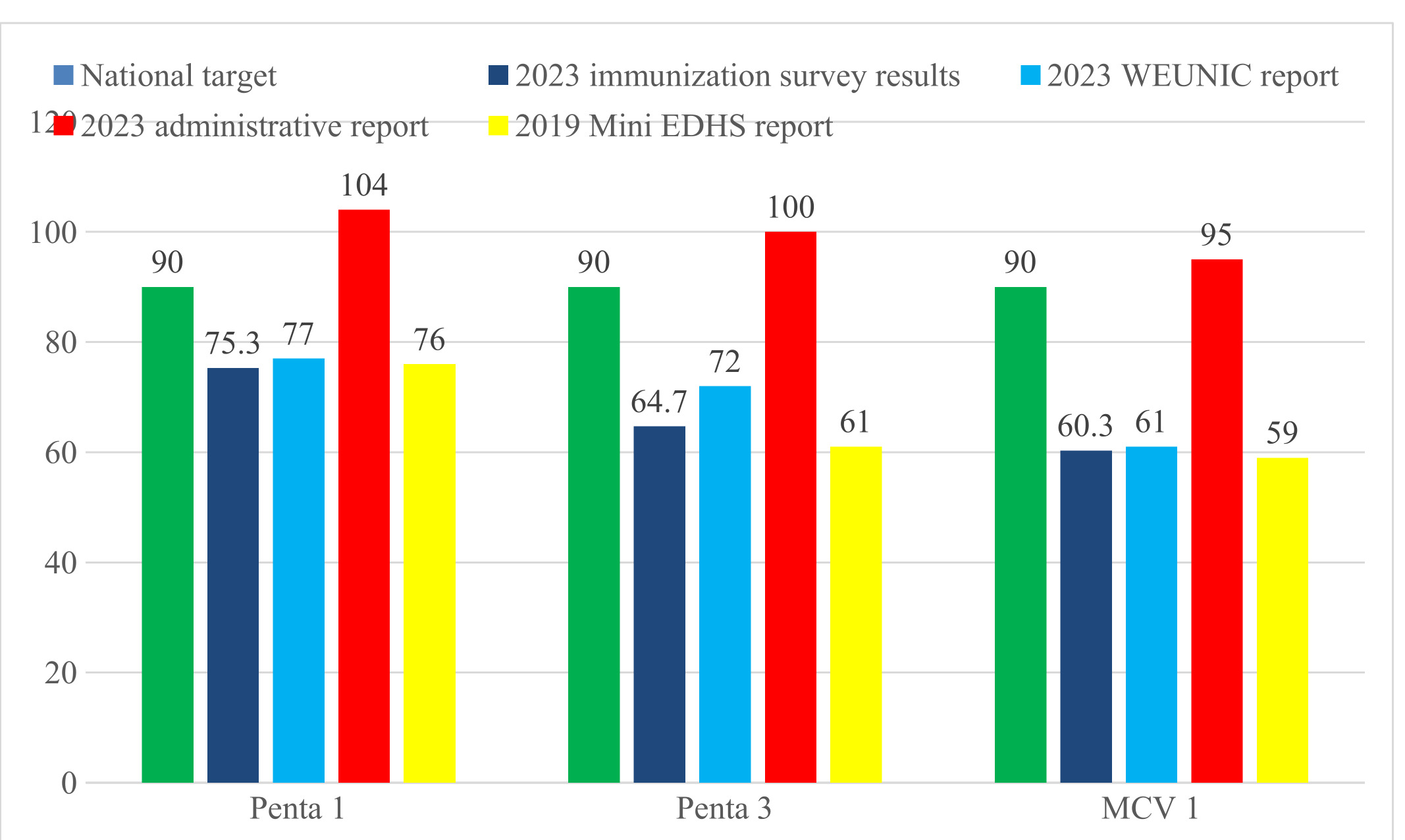
The study also reveals significant shortfalls in vaccination coverage compared to Ethiopia’s national target of 90% for all vaccines. These findings underscore the country’s challenges in meeting its immunisation goals, reflecting systemic issues within the vaccination program. When compared to the 2023 WEUNIC report24 and the 2019 Mini EDHS report,25 the survey highlights persistent barriers to achieving universal vaccine coverage. The finding also highlights high dropout rates in Penta and MCV vaccines, indicating difficulties in ensuring that caregivers complete their children’s full immunisation schedules. The potential reasons include geographic differences that can impact access to immunisation services, especially in areas affected by conflict or where people have a nomadic lifestyle, such as in pastoralist communities. These factors can disrupt immunisation service delivery and limit vaccination campaigns to address dropouts and missed communities. Additionally, a lack of cold chain equipment makes it difficult to store vaccines properly, especially in remote areas with weak healthcare systems.
To overcome these challenges, targeted actions are needed. Improving healthcare infrastructure, particularly in conflict zones, is crucial for ensuring reliable access to vaccines. Community engagement and education about the importance of completing vaccination schedules can help reduce dropouts. Involving local leaders and healthcare workers in outreach efforts can build trust and encourage caregivers to prioritise vaccinations. Addressing these issues requires a comprehensive approach that combines better infrastructure, logistical support, and community-based strategies.
In contrast, the 2023 administrative report shows coverage rates that exceed national targets, raising concerns about the reliability of the administrative reporting system. This gap between administrative data and survey findings suggests potential over-reporting, which may stem from outdated census-based target setting, inaccurate population estimates, or issues with data quality. The reliance on health facility reports for administrative data further exacerbates these discrepancies. These findings underscore the importance of targeted interventions, enhanced data quality control, and strengthened monitoring systems to reconcile administrative data with survey results and address the systemic challenges within Ethiopia’s immunisation program (Figure 6).
This study assessed HPV vaccination coverage among adolescent girls, revealing that over half had received the first dose of vaccine. This aligns with findings from various regional studies, including a systematic review that reported an overall coverage of 55%.26 However, the survey results indicate a lower coverage rate compared to the data released by the HPV information centre.27 This discrepancy may be because the HPV information centre data were collected from schools that didn’t account for all eligible girls who are not enrolled in school. The study further suggests that additional measures are necessary to increase the uptake of the HPV vaccine and achieve the national target of 90% or higher vaccination coverage.
The current study also revealed that half of the adult population had received at least one dose of the COVID-19 vaccine. This finding is consistent with other studies done in different parts of the country. The pooled estimates of the COVID-19 vaccine uptake showed that half of the respondents received the COVID-19 vaccine.28,29 The finding that half of the adult population received at least one dose of the COVID-19 vaccine underscores the importance of continued public health efforts to enhance vaccination uptake. While this aligns with national trends, it suggests that a significant portion of the population remains unvaccinated, which can impact herd immunity and overall public health. To improve coverage, targeted outreach, education, and accessibility initiatives are necessary, particularly in underserved areas, to ensure higher vaccination rates and mitigate the impact of future COVID-19 variants.
This nationally representative study offers valuable insights into life-course vaccination coverage in Ethiopia, marking the first assessment of its kind. Although a large sample was obtained, the exclusion of certain sites, particularly the Tigray region, due to ongoing conflict would underrepresent national vaccination coverage in conflict-affected regions. Despite this, the study represents more than 90% of the country and provides important insights into the overall status of vaccination coverage nationwide.
CONCLUSIONS
This study revealed that the uptake of childhood immunisation services was found to be suboptimal for all types of vaccines. Nationally, one out of four children did not receive any vaccines at all. In addition, only nearly four in ten children completed the full course of recommended doses. Furthermore, among those who began vaccination services, nearly one in two children dropped out before reaching the pentavalent3 and MCV1 stages, respectively. Immunisation coverage also varies significantly across different regions. This highlights the importance of implementing region-specific interventions and approaches tailored to the specific contexts.
The national maternal vaccination coverage for Tetanus Toxoid-Diphtheria (Td) was high, indicating that most mothers have received at least one dose of the Td vaccine. However, almost four in a hundred mothers completed the full dose of the Td vaccine. Furthermore, approximately half of adolescent girls received at least one dose of the HPV vaccine, and only a quarter of adolescents received the second dose. More than half of adults received at least one dose of the COVID-19 vaccine. Nearly one in four individuals had received the second dose of the COVID-19 vaccine.
The key points that could be recommended to address the gaps across the regions are working on vaccine availability and properly approaching clients, which can help to enhance the service uptake of immunisation services, since the coverage of zero doses and dropouts is substantially high, applying digital microplanning and collecting the geo tagged data of children may help to track zero dose children and defaulters properly. Finally, designing a digital demand generation and communication system may also help users access relevant information and minimise vaccine hesitancy to improve life course immunisation service uptake.
ACKNOWLEDGEMENTS
We thank the CBMP Consortium Universities for their technical support and Amref Health Africa for financial assistance. We also acknowledge WHO, UNICEF, JSI, and PATH for logistical support. We extend our appreciation to the Ministry of Health, Regional Health Bureaus, Zonal and Woreda Health Offices, health facilities, and health posts for their collaboration. Finally, we sincerely thank the participating communities, mothers/caregivers, and health workers for their valuable contributions.
DISCLAIMER
The views and opinions expressed in this article are those of the authors and do not necessarily reflect the official policies or positions of the Ministry of Health or any other partner institution.
ETHICS STATEMENT
The study adhered to the principles outlined in the Declaration of Helsinki. Ethical approval was granted by the Institutional Review Board of Hawassa University (IRB/288/15). Support letters were obtained from the Ministry of Health and the Regional Health Bureaus. Written informed consent was obtained from all participating mothers/caregivers and vaccinators. Data were collected anonymously using the ODK system to ensure confidentiality.
DATA AVAILABILITY
The data underlying this article are available from the corresponding author upon reasonable request. Due to institutional and ethical data-sharing policies, the dataset is not publicly accessible.
FUNDING
This study was financially supported by Amref Health Africa, with additional financial and logistical contributions from UNICEF, WHO, JSI, and PATH. The funders had no role in the design of the study, data collection, data management, analysis, interpretation of the findings, manuscript writing, or the decision to submit the article for publication.
AUTHORSHIP CONTRIBUTIONS
BFE, GA, YA, BD, AT, AA, MAu, KG, GT, SS, BT, and KA conceptualised and designed the study, contributed to data analysis and interpretation, prepared the first draft of the manuscript, supervised data collection, validated the findings, and critically revised and edited the manuscript.
MM, NW, MN, YL, MZ, and MY contributed to study conceptualisation, conducted formal data analysis, supported data curation and resource coordination, reviewed and edited the manuscript, and supervised data collection. All authors reviewed and approved the final manuscript and agreed to be accountable for all aspects of the work.
DISCLOSURE OF INTEREST
The authors completed the ICMJE Disclosure of Interest Form (available upon request from the corresponding author) and disclose no relevant interests.
ABBREVIATIONS
ANC – Antenatal Care
BCG – Bacille Calmette–Guérin
BSc – Bachelor of Science
CBMP – Capacity Building and Mentorship Partnership
CI – Confidence Interval
COVID-19 – Coronavirus Disease 2019
DPT – Diphtheria–Pertussis–Tetanus
EA/EAs – Enumeration Area(s)
EDHS – Ethiopian Demographic and Health Survey
EPI – Expanded Programme on Immunisation
ESS – Ethiopian Statistical Services
GPS – Global Positioning System
HPV – Human Papillomavirus
ICC – Immunisation Interagency Coordinating Committee
IRB – Institutional Review Board
LMICs – Low- and Middle-Income Countries
MCV – Measles-Containing Vaccine
MCV1 – First Dose Measles-Containing Vaccine
MCV2 – Second Dose Measles-Containing Vaccine
MoH – Ministry of Health
MPH/MSc – Master of Public Health / Master of Science
NITAG – National Immunisation Technical Advisory Group
ODK – Open Data Kit
OPV – Oral Polio Vaccine
PCV – Pneumococcal Conjugate Vaccine
SD – Standard Deviation
SDG – Sustainable Development Goal
SNNP – Southern Nations, Nationalities and Peoples Region
Td – Tetanus–Diphtheria
ToT – Training of Trainers
TWG – Immunisation Technical Working Group
VPD – Vaccine-Preventable Disease
WHO – World Health Organisation