Health commodity supply chains constitute a fundamental pillar of health systems, as they determine the continuous availability of essential medical inputs, patient safety, and overall quality of care. Their functioning also affects the economic efficiency of health systems by limiting losses, stock-outs, and avoidable costs associated with emergency procurement or expired products.1,2
In low- and middle-income countries, supply chain performance remains a major challenge due to persistent structural constraints, including limited financial resources, weak planning capacity, transport bottlenecks, and institutional fragmentation.3
In Benin, health commodity supply chains experience recurrent dysfunctions, particularly at the “last mile” level. According to national guidelines, nearly seven out of ten health facilities reported at least one stock-out among tracer products monitored over a six-month period.4 Supply, which is generally conducted on a monthly basis, remains highly dependent on the availability of financial, human, and logistical resources at peripheral levels.
Most health zones operate under a PULL model, in which health facilities initiate orders based on their consumption patterns. Although this model theoretically aims to improve alignment with local demand, it proves vulnerable in contexts characterised by limited quantification capacity, weak supervision, and inadequate transport systems, resulting in prolonged lead times, frequent stock-outs, and substantial logistical losses.1,3
In response to these limitations, several countries have experimented with PUSH models based on centralised planning and demand anticipation, with the objective of improving supply reliability, reducing stock-outs, and optimising logistics costs. These experiences, particularly in sub-Saharan Africa, have demonstrated positive outcomes, including marked improvements in overall supply chain performance.5
In Benin, where both models coexist depending on programmes and health zones, rigorous comparative analyses remain scarce. It is within this context that the present study was conducted in 2025 in the Couffo Department.
The objective of this study was to assess the technical and economic contribution of the PUSH model to health commodity supply chain management. The Couffo department was selected for the study given that it represents the unique setting in which both the PUSH and PULL supply models operate concurrently, alongside strong comparability of the health zones implementing them.
METHODS
Study setting
The study was conducted in the Couffo Department, which comprises six municipalities and includes 65 public health facilities organised into two health zones: the Kloukékanmè–Toviklin–Lalo (KTL) health zone and the Aplahoué–Djakotomey–Dogbo (ADD) health zone. These zones share similar demographic, institutional, and logistical characteristics, ensuring their comparability.
Study design and sampling
This was a descriptive cross-sectional study with evaluative and analytical purposes. It was based on a comparison between the Kloukékanmè–Toviklin–Lalo (KTL) health zone, which had adopted the PUSH model (centralised and planned supply) and was therefore considered the intervention area, and the Aplahoué–Djakotomey–Dogbo (ADD) health zone, which applied the PULL model (demand-based supply) and was considered the control area.
The study population consisted of public health facilities (health centres and district warehouses), professionals involved in logistics management (facility managers, logisticians, and Expanded Programme on Immunisation [EPI] focal persons), as well as patients attending the facilities during the data collection period.
-
Inclusion criteria: health facilities operational for at least six months and staff members in post who consented to participate.
-
Exclusion criteria: newly opened or temporarily closed facilities, and staff members who were unavailable or did not provide consent.
-
Sampling: 50% of health facilities were randomly selected, corresponding to 32 centres in total (16 per health zone). Both district warehouses were included exhaustively.
Variables and measurement
Two groups of variables were examined:
-
Independent variables: elements characterising the implementation components of each logistics model applied (PUSH or PULL).
-
Dependent variables: overall supply chain effectiveness, assessed through indicators such as product availability, reduction in lead times, stakeholder and community satisfaction, reduction in logistics costs, and reduction in losses.
Each logistics system component was broken down into operationalised sub-components, with coded criteria (score of 0 or 1 depending on absence or presence, with higher weighting for major criteria). The components included:
-
Inputs: human, material, financial, and information resources.
-
Processes: procurement, storage, distribution, and quality assurance.
-
Outcomes: availability, compliance, satisfaction, costs, and spoilage.
Scores were converted into proportions (%) and interpreted using the Varkevisser scale: good performance ≥ 80%, poor performance < 80%. This scale is a recognised standard tool within health systems for assessing programme performance, particularly in African contexts, and whose simplicity facilitates standardisation.
Data collection
Data were collected from 17 March to 15 April 2025 using observation checklists in warehouses and health facilities, and interview guides for professionals and patients (perceived availability experience). Normative and operational documents (guidelines, registers, order forms, and logistics reports) were systematically reviewed.
The data covered the period from September 2024 to February 2025.
Data analysis
Data processing and analysis were conducted manually and using Stata version 14. The analysis comprised:
-
descriptive phase: categorisation, transcription, and presentation of component-level scores.
-
analytical phase: inter-zone comparisons using Student’s t-test and chi-square tests at a 5% significance level; logistic and linear regression analyses were performed depending on the nature of the variables, with estimation of odds ratios (ORs) and coefficients (β).
Furthermore, it should be noted that composite indicators (such as overall performance) are derived from aggregated scores combining responses from different categories of participants in order to reflect a multidimensional perspective. Regression analyses were conducted using indicators specific to each type of respondent. Normality of residuals, homoscedasticity, and multicollinearity were verified for the linear regression models.
Ethical considerations
The study was conducted in accordance with ethical principles. The protocol was reviewed and approved by an IRSP ethics committee, which authorised compliance with ethical requirements. Formal authorisations were obtained from the Ministry of Health and subsequently from the Couffo Departmental Health Directorate prior to data collection. Informed consent was obtained from all participants after explanation of the study objectives, and confidentiality and anonymity were strictly ensured throughout all stages of the study.
RESULTS
Description of the study population
The study included 176 participants distributed across the two health zones of the Couffo Department: ADD (Aplahoué–Djakotomey–Dogbo) and KTL (Kloukékanmè–Toviklin–Lalo). The units of observation comprised 32 public health centres (16 in each health zone), two district warehouses, 32 facility managers, 32 Expanded Programme on Immunisation (EPI) focal persons, 2 district logisticians and 110 patients interviewed by convenience sampling (55 per zone). All selected health centres had been operational for more than six months.
Assessment of logistics components
The analysis highlights differing levels of implementation of logistics system components in the ADD and KTL health zones over the previous six months.
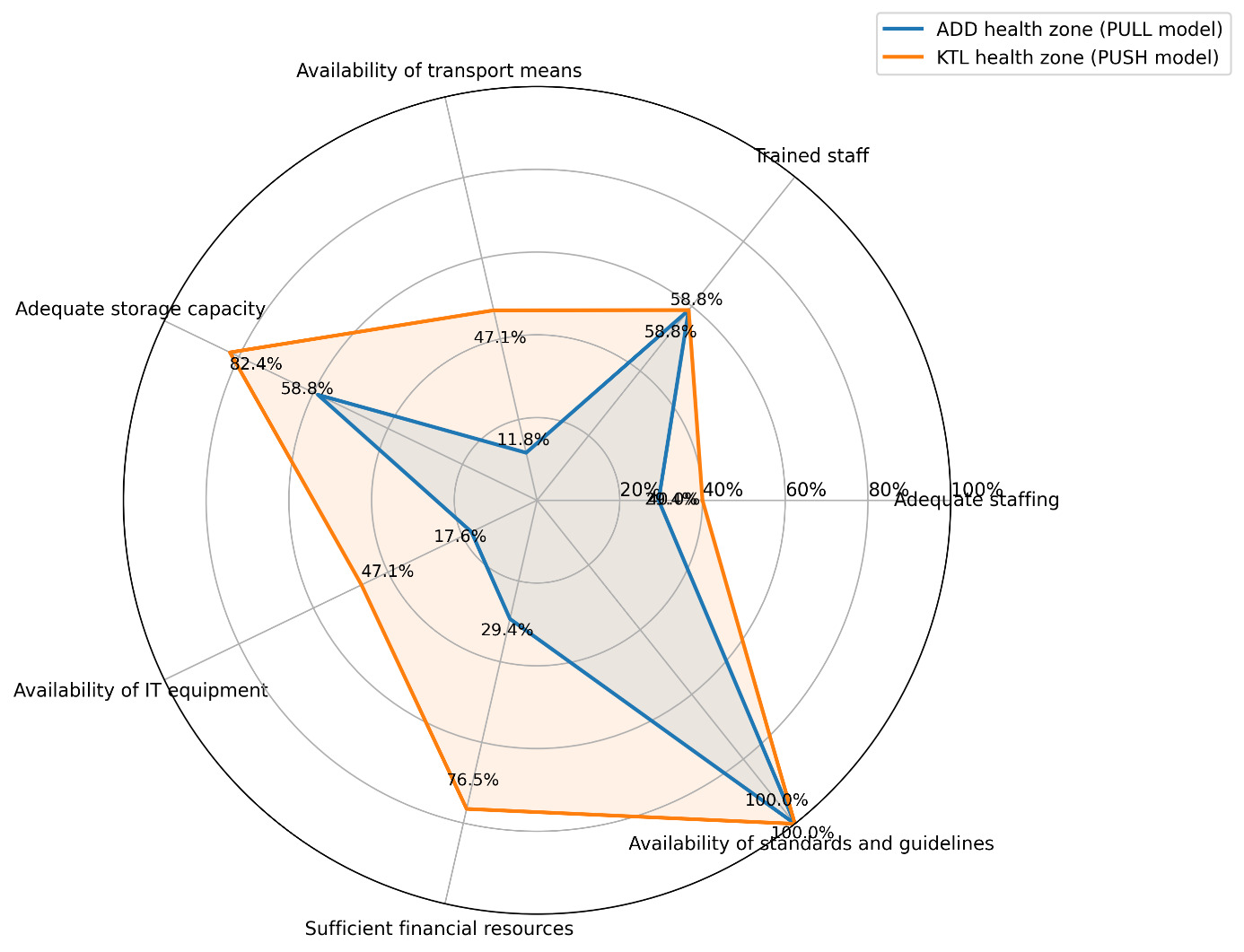
In the ADD health zone, logistics resources were generally limited. Only 29.40% of facilities reported having sufficient staff, and 64.70% reported that staff were trained. Material resources were also limited, with low availability of transport means (5.90%) and information technology equipment (35.30%) (Figure 1). Storage capacity was considered adequate in 58.80% of facilities. Financial resources were deemed sufficient by 29.40% of facilities, while logistics standards and guidelines were available in all facilities (100%).
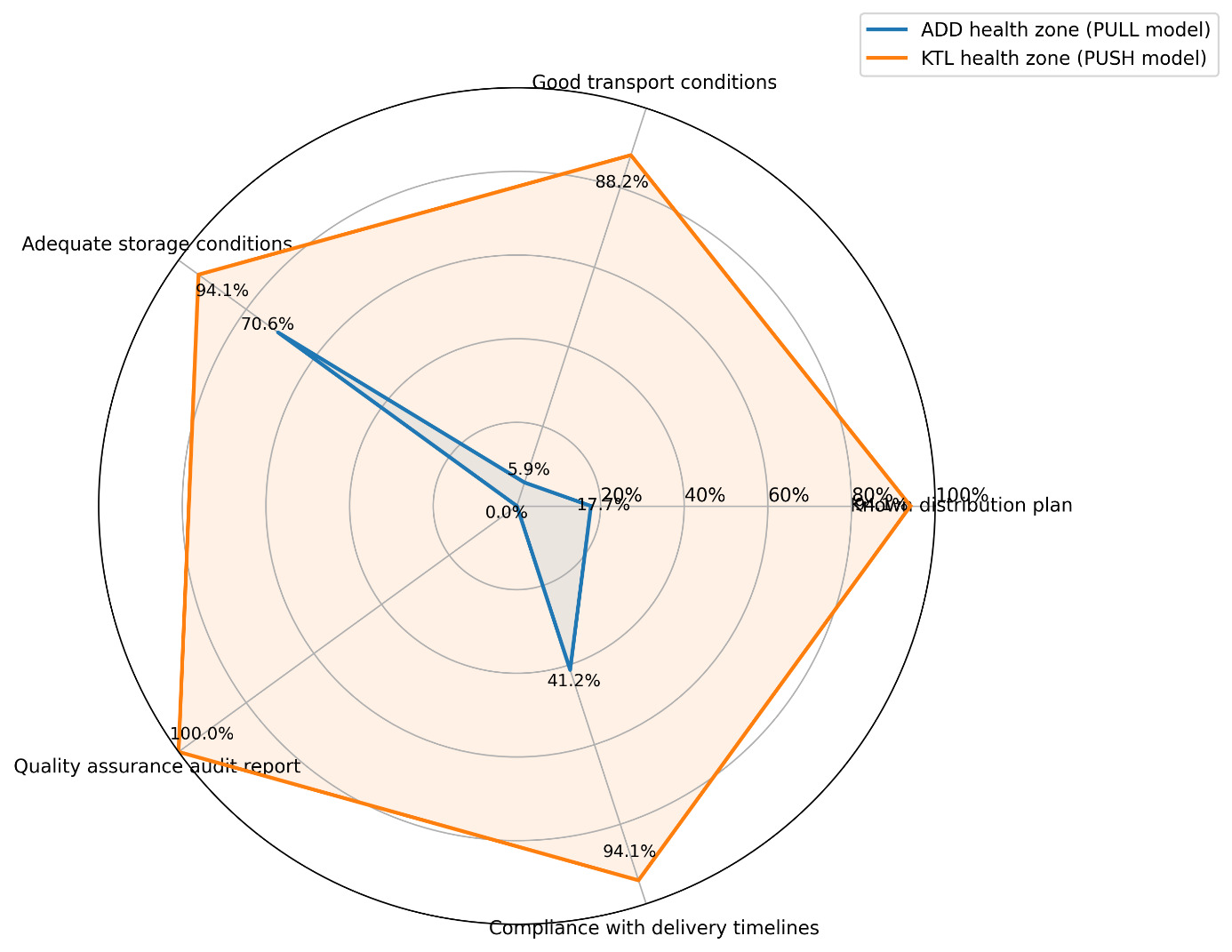
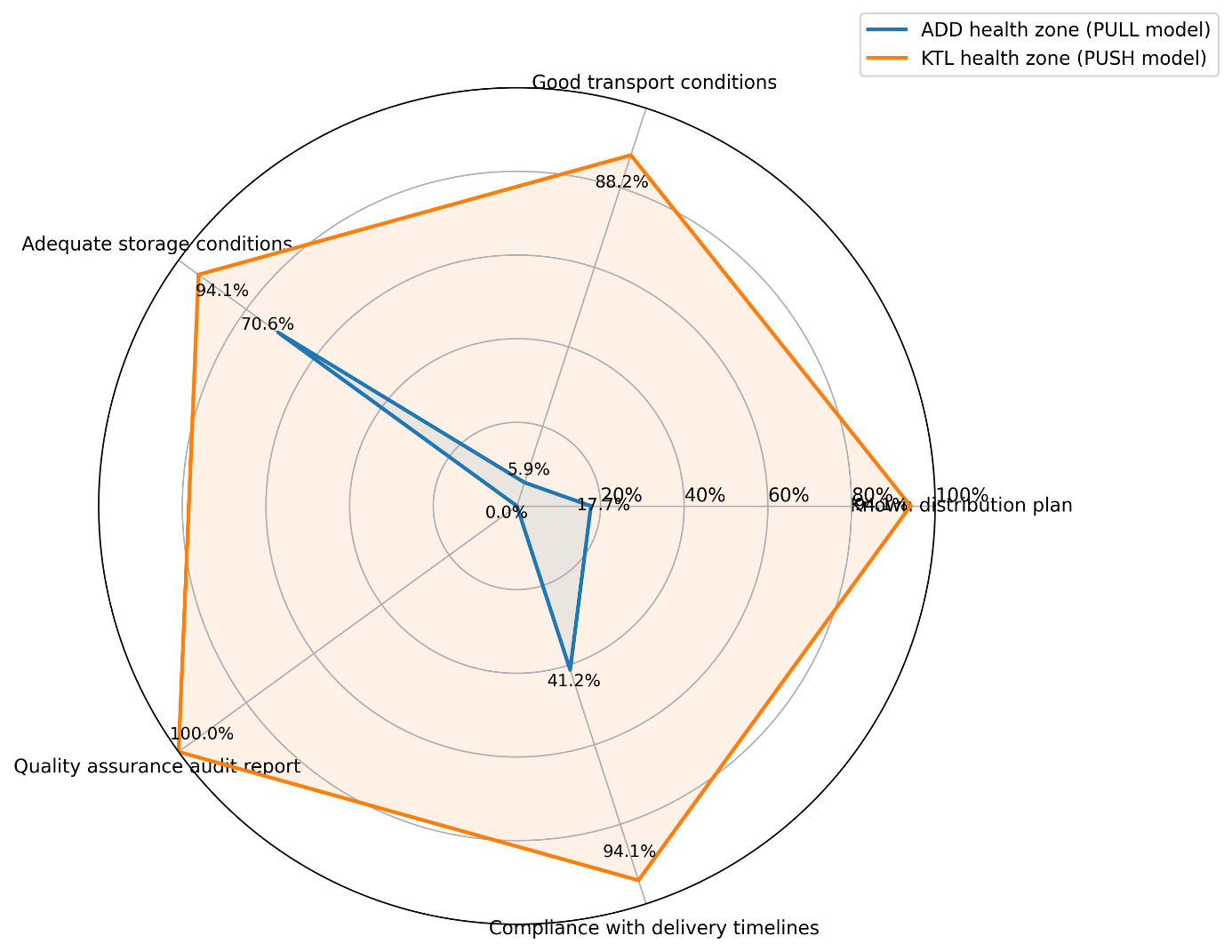
Figure 2 shows that logistics processes in the ADD zone were weakly structured: limited awareness of distribution plans (17.70%), transport conditions rarely considered satisfactory (5.90%), near absence of quality assurance audits (0%), and low compliance with delivery timelines (41.2%). Storage conditions, however, were considered adequate in 70.60% of facilities.
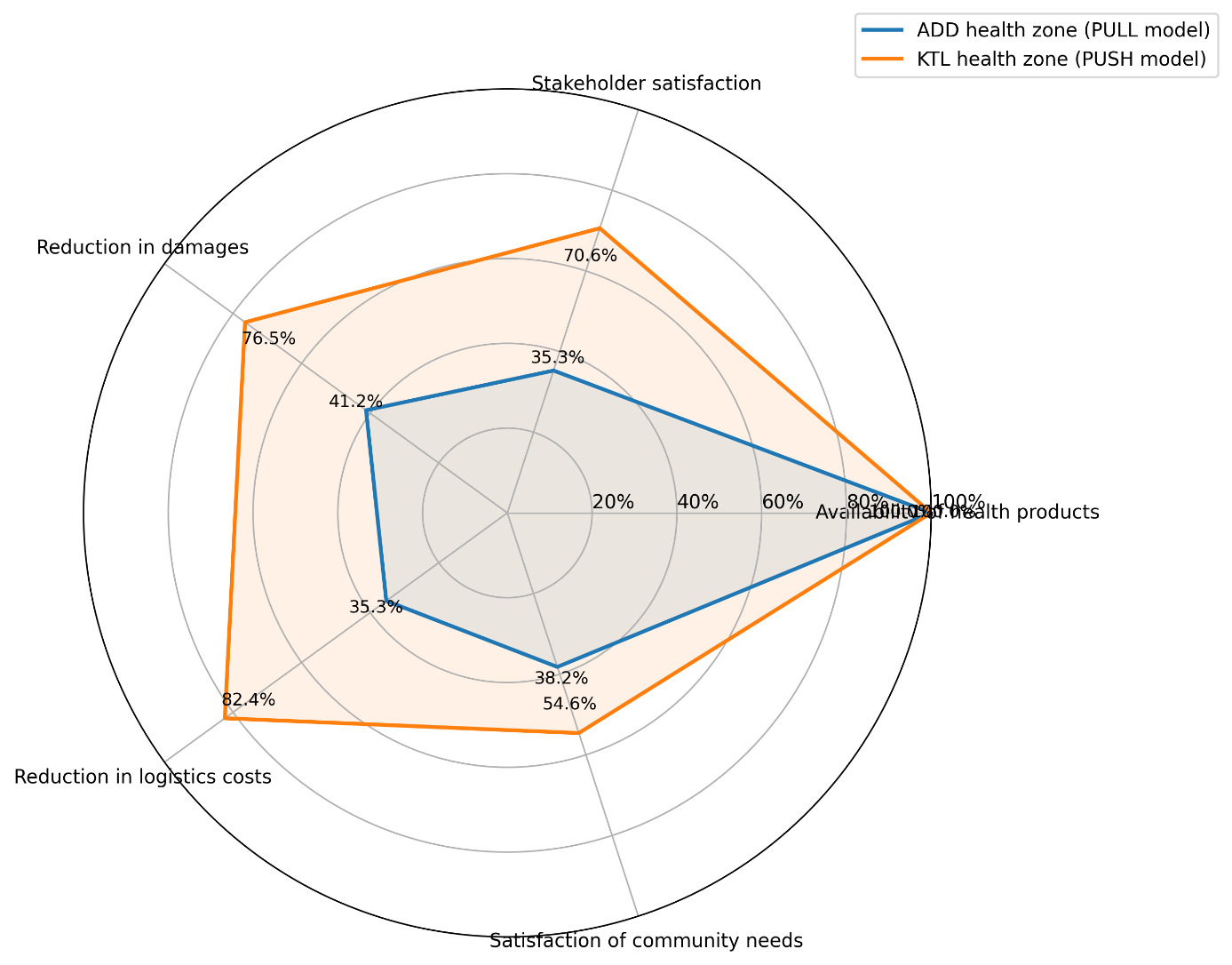
Regarding outcomes (Figure 3), health product availability was reported in all facilities (100%). However, only 35.3% of stakeholders reported satisfaction, 41.2% reported a reduction in spoilage, 35.3% reported a decrease in logistics costs, and 38.2% considered that community needs were adequately met.
By contrast, the KTL health zone demonstrated better performance. Resources were more readily available, particularly transport means (47.1%), information technology equipment (47.1%), storage capacity (82.4%), and sufficient financial resources (76.5%). Logistics processes were better organised, with widespread knowledge of distribution plans (94.1%), satisfactory transport conditions (88.2%), quality assurance audits conducted in all facilities (100%), and high compliance with delivery timelines (94.1%). These performances translated into more favourable outcomes, including higher stakeholder satisfaction (70.6%), reduced spoilage (76.5%), lower logistics costs (82.4%), and improved satisfaction of community needs (54.6%) (Figure 3).
_component_of_the_health_supply_chain_in_add_and_ktl_health_zones.png)
_component_of_the_health_supply_chain_in_add_and_ktl_health_zones.png)
Analysis of contributions to overall performance
Logistics performance indicators
Over the past six months, the KTL health zone has demonstrated better logistics performance than the ADD zone (Table 1). The availability of tracer products was higher in KTL (98.8% vs 94.16%), with a greater proportion of health facilities experiencing no stock-outs (88.23% vs 52.94%). Losses related to expired or spoiled products were substantially lower in KTL (14.98% vs 36.27%), as was the presence of expired products per facility (46.66% vs 70.6%).
Community satisfaction (54.54% vs 38.2%) and stakeholder satisfaction (70.58% vs 33.33%) were also higher in KTL, alongside a shorter average delivery lead time (9 days compared with 21 days). Taken together, these indicators suggest that the PUSH model implemented in KTL improves supply reliability, limits losses, and strengthens stakeholder satisfaction.
Comparative statistical analysis
The evaluation of the PUSH model using logistic regression analyses shows a significant effect on several key dimensions of logistics performance (Table 2). The model reduces the risk of stock-outs, improves perceived product availability, and substantially decreases the average delivery lead time by nearly 13 days. It doubles the likelihood of product availability, reduces the duration of stock-outs by almost 10 days, and has a strong effect on lowering logistics costs and improving stakeholder satisfaction within the supply chain.
The observed effects on the reduction in spoilage and on patient satisfaction were not statistically significant, indicating favourable trends that require confirmation with additional data. Overall, these results support the hypothesis that the PUSH model enhances the overall efficiency of the supply chain.
Comparison of logistics costs
Over the period from September 2024 to February 2025, logistics costs were significantly lower in the KTL health zone (PUSH model) compared to ADD (PULL model) (Table 3). The average cost of procurement operations was USD 10.86 in KTL versus USD 12.71 in ADD (p=0.018). Monthly transport costs were more than threefold lower in KTL (USD 2.60 vs. USD 8.41; p<0.001), as was the cost per kilometre (USD 0.30 vs. USD 1.33; p<0.001). These findings demonstrate substantial economic efficiencies associated with the PUSH model, particularly in transport optimisation. (Exchange rate: 1 USD=600 FCFA).
DISCUSSION
The findings of this comparative study between the KTL health zone (PUSH model) and the ADD health zone (PULL model) in the Couffo Department provide important insights into the implications of supply chain management for health system performance. The discussion is structured around an assessment of system components, the specific contributions of the PUSH model, the practical implications of the findings, and the study limitations.
Assessment of the implementation of Inputs, Processes, and Outcomes components
Analysis based on the classical Structure–Process–Outcome framework inspired by Donabedian highlights marked differences between the two health zones, which largely explain the observed performance gaps.6
The KTL zone (PUSH) benefits from greater availability of critical resources, including transport means, information technology equipment, and financial resources. Such availability constitutes a fundamental prerequisite for an effective supply chain and remains a persistent challenge in health systems in low- and middle-income countries.7,8 By contrast, the ADD zone (PULL) suffers from structural constraints, particularly in trained personnel and transport equipment, which hinder the implementation of robust logistics processes.
Logistics processes in KTL appear to be more advanced. The existence and operationalisation of a formal distribution plan, the systematic conduct of quality assurance audits, and high compliance with delivery timelines reflect a proactive and controlled logistics system, characteristic of optimised PUSH models.9,10 In ADD, weak process performance, limited awareness of distribution plans and the absence of audits, illustrates the shortcomings of a reactive PULL system, which relies heavily on the initiative capacity of individual facilities, often under constrained conditions.
These differences in inputs and processes are directly reflected in outcomes. Although physical product availability is reported at 100% in both zones, quality-related indicators such as reductions in spoilage, lower logistics costs, and higher levels of stakeholder and community satisfaction are significantly better in KTL. This finding confirms that nominal availability alone is insufficient; the quality of logistics management directly influences economic performance and users’ perceptions.11,12
Contributions of the PUSH model to supply chain performance
Contributions to logistics performance
The results demonstrate that the implementation of the PUSH model is significantly associated with key logistics performance indicators. It appears to result in a substantial reduction in the risk of stock-outs (OR=0.21), an increase in perceived product availability (OR=2.00), and a reduction of nearly 13 days in the average delivery lead time, representing major improvements observed in the KTL zone. These findings are consistent with international evidence indicating that PUSH models, particularly those implemented as “delivery team topping up” or “informed push” systems, help secure last-mile supply by reducing dependence on local ordering capacity.9,10,13
These contributions may be explained by centralised planning and regular pre-scheduled deliveries, which reduce variability and uncertainty, thereby limiting the “bullwhip effect” commonly observed in fragmented supply chains.14 By reducing stock-outs, the PUSH model also contributes to improved utilisation of health services and continuity of care, as previously demonstrated by Kuwawenaruwa et al. and Mukundiyukuri et al.11,15
The marked reduction in losses (from 36.27% to 14.98%) and expired products in KTL further suggests improved stock management and more efficient inventory rotation, in line with recommended practices for reducing wastage.16,17 These results are consistent with evidence from Senegal and several East African countries, where the protective effect of PUSH models or centrally managed and supervised logistics processes on stock management and product rotation has been highlighted.10,16,17
Contributions to economic performance (logistics costs)
The economic analysis reveals a clear advantage of the PUSH model. The significant reduction in total logistics costs (OR=8.56), and more concretely the more than threefold reduction in average monthly transport costs and cost per kilometre in KTL, provide compelling evidence of improved efficiency. This economic performance likely stems from centralised planning, route optimisation, consolidation of flows, and better utilisation of transport resources, particularly through pooling mechanisms—thus generating substantial economies of scale within health commodity supply chains.18–20
Whereas under the PULL model in ADD, transport costs were higher and more variable (as reflected by the large standard deviations), likely due to emergency and uncoordinated orders, the PUSH model in KTL seems to enable efficient resource planning, transforming logistics from a cost centre into a lever for budget optimisation. In this way, the PUSH model may convert dispersed and variable costs into controlled and predictable expenditures, thereby improving overall system efficiency.
In a context characterised by the predominance of direct financing of health facilities, as highlighted by Ruhago et al.,21 reducing logistics costs represents a critical lever for strengthening the financial sustainability of health facilities and alleviating the financial burden on service users.
Implications of the findings
The implications of this study are multifaceted. From an operational perspective, the findings support strengthening and scaling up the PUSH model (proactive planning, regular deliveries, and quality control) within the Beninese health system, particularly at the last-mile level, in line with national guidelines.4 This approach is consistent with recommendations advocating broader integration of supply chains, notably for vaccines and other health commodities.22,23
Investment in key structural resources (human resources, training, transport assets, and information systems), alongside the standardisation of logistics processes, emerges as a critical prerequisite for sustaining high-performing supply chain operations.
From a policy perspective, the substantial savings achieved in logistics costs provide a strong justification for initial investments. Reductions in losses and stock-outs directly contribute to the goal of equitable and efficient access to essential medicines, a cornerstone of resilient health systems.1,24 Furthermore, the improved satisfaction of stakeholders observed in the KTL zone (OR=4.40) may enhance staff motivation, ownership, and long-term adherence to good logistics practices.14
Study limitations
This study has several limitations. First, its observational and cross-sectional design does not allow definitive causal inference. Second, the scope was restricted to two health zones within a single department, which limits the generalisability of the findings to other regions. Third, certain contextual factors (such as local leadership and team dynamics) that may influence performance were not captured. Fourth, social desirability bias in the satisfaction interviews and the subjectivity of observation could affect the robustness of the findings.
The lack of statistical significance observed for patient satisfaction and reduction in spoilage indicates the need for studies with larger sample sizes or more sensitive measurement tools. Finally, the economic evaluation could be strengthened by more comprehensive costing analyses that incorporate long-term health outcomes, which would provide valuable guidance for decision-makers.25
Despite these limitations, the convergence of descriptive, analytical, and economic results reinforces the strategic relevance of the PUSH model for improving the performance and efficiency of the health logistics system in Benin.
CONCLUSIONS
This comparative study demonstrates that the PUSH model (planned and proactive supply) is associated with logistical and economic performance that is higher than in the PULL model, with significant benefits across several management and stakeholder satisfaction indicators.
The model represents a cost-effective strategic investment, generating substantial efficiency gains through reductions in operational costs (particularly transport) and financial losses due to expired products. From a logistics standpoint, it seems to improve availability of essential medicines and greater reliability of the supply chain.
Overall, the findings show that, despite persistent structural challenges, optimising core supply chain processes can yield substantial logistical and economic gains that satisfy both stakeholders and communities. They strongly support scaling up the PUSH model, a proactive approach in which logistics is viewed as a critical lever for improving the efficiency of health expenditure and equity in access to care. Nevertheless, further in-depth studies are required to consolidate these gains and to monitor the long-term sustainability of the performance improvements induced by this model.
Acknowledgements
The authors are grateful to IRSP-CAQ, the Ministry of Health, and the staff of the Couffo Departmental Directorate of Health, as well as the coordination teams and health-zone staff of KTL and ADD, for their valuable support and collaboration.
Disclaimer
The views expressed in this article are those of the authors and do not necessarily represent the official position of their institutions.
Ethics statement
This study was approved by the Ethics Board of the Regional Institute of Public Health (IRSP). Informed consent was obtained from all participants prior to data collection. Confidentiality and anonymity were strictly maintained throughout the study.
Data availability
The datasets generated and analysed during the current study are available from the corresponding author upon reasonable request.
Funding
The research presented in this manuscript received no external funding.
Authorship contributions
All authors meet the ICMJE authorship criteria, contributed significantly to the work, and approved the final version of the manuscript.
Disclosure of interest
The authors completed the ICMJE Disclosure of Interest Form (available upon request from the corresponding author) and disclose no relevant interests.
Correspondence to:
Lamidhi SALAMI
Institut Régional de Santé Publique
Université d’Abomey-Calavi
Bénin
s.lamidhi@yahoo.com