The need for obstetric care is defined in terms of health conditions that require appropriate medical management.1 It is an indicator that supports political, social, and professional awareness for planning and development of strategies aimed at reducing the maternal mortality ratio.2 Reducing maternal mortality in developing countries remains a major challenge, as maternal mortality ratios are, on average, eighteen times higher than in developed countries and, despite ongoing efforts, show little evidence of decline.3 The World Health Organization estimates that 40% of all pregnant women experience some form of pregnancy-related complication.4 Furthermore, barriers to accessing essential basic and emergency obstetric care constitute a significant contributor to maternal and infant morbidity and mortality.5
The 2014 Multiple Indicator Cluster Survey (MICS) reported a maternal mortality ratio of 452 per 100,000 live births in Haut-Katanga Province.6 Maternal deaths were primarily associated with direct obstetric causes, including obstetric haemorrhage (23.4%), hypertensive disorders (16.9%), abortion-related complications (11.1%), infections (10.2%), embolism, and other direct causes (10.8%),6 while only 26.7% were attributable to indirect causes.7 Data from the Democratic Republic of Congo’s Health Information System (DHIS2) between 2019 and 2022 indicate persistently high maternal mortality ratios in several health zones, with variations in underlying causes across facilities depending on socio-economic, geographical, and cultural contexts, as well as the organisation of health services.8
The literature on this emerging approach to assessing unmet obstetric needs in the Democratic Republic of Congo remains limited. Apart from a study by Tambue MA et al. (2011) on the availability, utilisation, and quality of emergency obstetric and neonatal care in Lubumbashi—which demonstrated limited availability of such services, with only one tertiary facility, Jason Sendwe Hospital, providing the full set of nine signal functions9—and a study by Ngandu MV (2019), which reported that only 21.1% of obstetric needs were met compared with 77.9% unmet needs, alongside a caesarean section rate of 1.4% across the former Katanga Province, evidence remains scarce.10
The limited availability of literature in the Democratic Republic of Congo on this approach prompted us to conduct this study to assess the coverage and magnitude of unmet obstetric needs in Lubumbashi, identify factors associated with maternal mortality, and evaluate stakeholders’ awareness of this approach.
Methods
Study setting and design
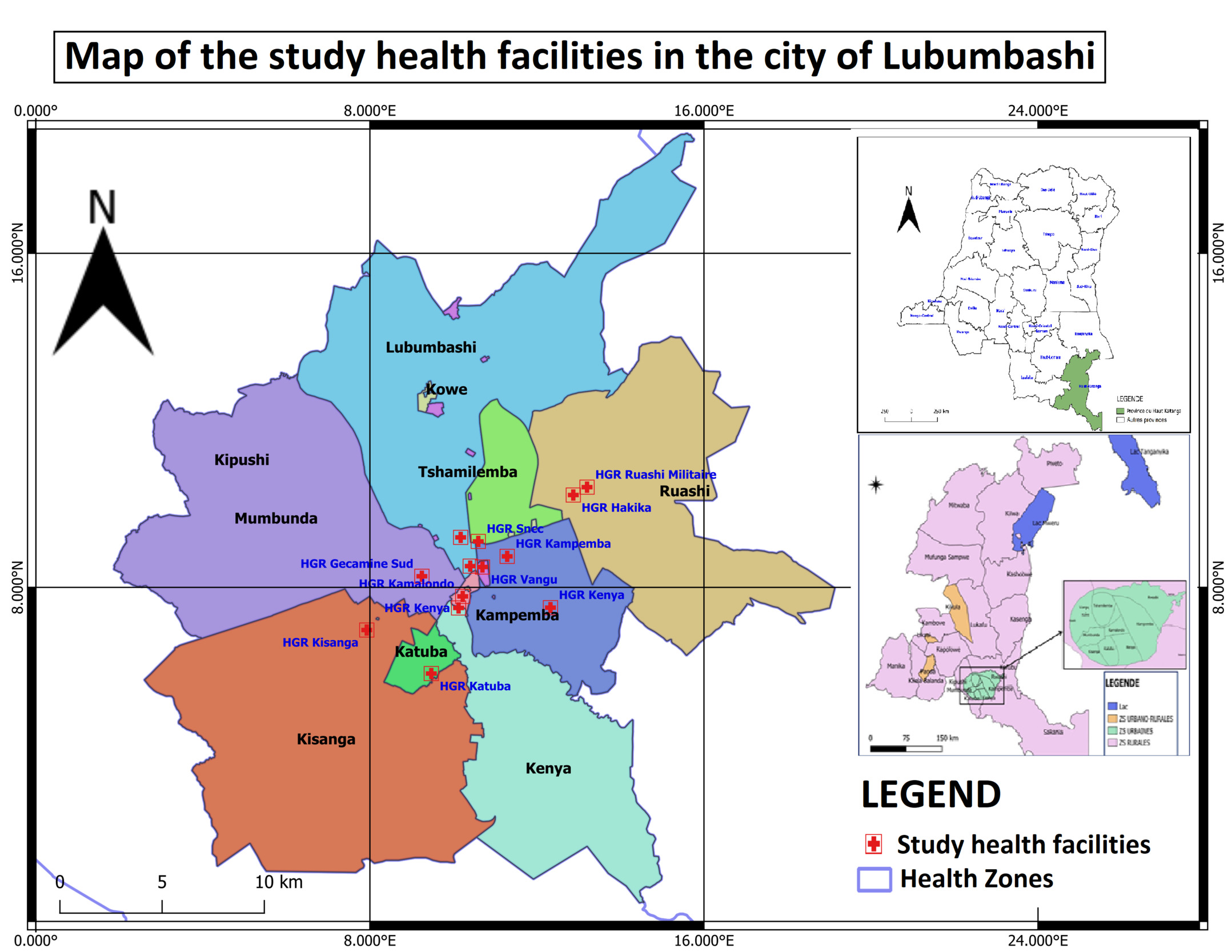
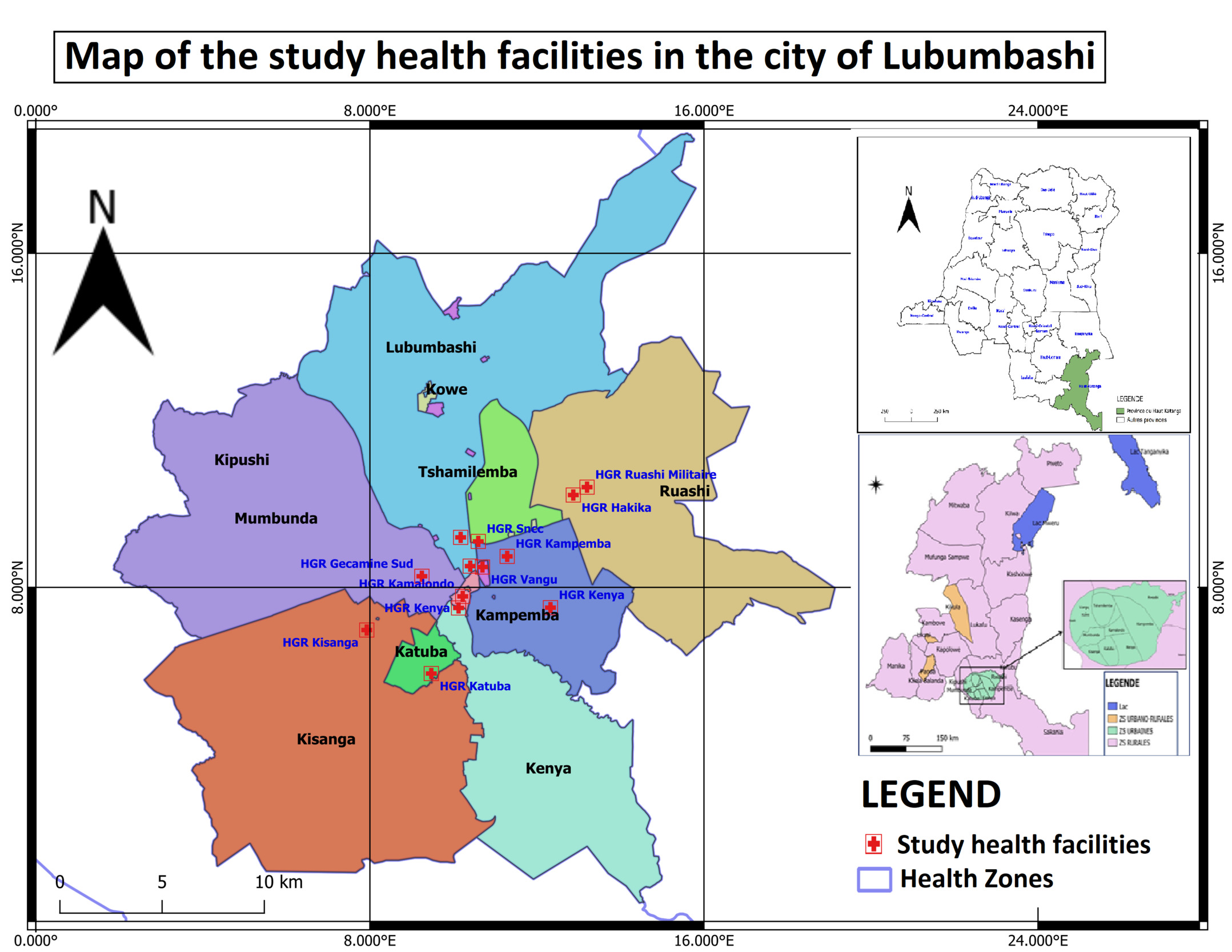
A mixed-methods cross-sectional analytical study with a phenomenological qualitative component was conducted in 12 health facilities in Lubumbashi, including 10 secondary-level facilities and 2 tertiary-level institutions, namely the University Clinics and the Provincial Jason Sendwe Hospital. The study spanned four years (2019–2022) for the retrospective collection of quantitative data, while semi-structured interviews were conducted in 2023.
Study population and sampling
The sample size was calculated using Cochran’s formula. In this formula, p represents the proportion of women experiencing complications during childbirth according to WHO estimates (10% in 2022), Zα was set at 1.96 for a 95% confidence interval, and the margin of error (d) was set at 5%.
or Additionally, 30 semi-structured individual interviews were conducted with healthcare professionals. Source triangulation was applied, and interviews were carried out until data saturation was achieved.
Data Collection and Analysis
Data were obtained from the electronic database of the National Health Information System (SNIS) through DHIS2 and from documentary review using an electronic questionnaire developed in Open Data Kit (ODK). For the qualitative component, data were collected using a semi-structured interview guide and audio recording.
Data management was performed using Microsoft Excel 2019, while statistical analyses were conducted using RStudio and SPSS version 26.0. Mapping was carried out using QGIS. Depending on data distribution, appropriate statistical tests were applied, with p-values calculated at a significance level of α = 5%. Logistic regression analysis was performed to identify types of major obstetric interventions associated with maternal mortality. Adjusted odds ratios (aOR) with their corresponding 95% confidence intervals (95% CIs) were reported to measure the strength of association between independent variables and the outcome. The overall goodness-of-fit of the model was assessed using the Hosmer–Lemeshow test, and model specification was verified using the link test. Qualitative data were analysed using a deductive thematic approach with ATLAS.ti version 7.3.15.
Inclusion Criteria
This study included pregnant women admitted between 1 January 2019 and 31 December 2022 for either absolute or non-absolute maternal indications and who had complete medical records in public secondary- and tertiary-level health facilities in the city of Lubumbashi.
For the qualitative component, participants included officials from the Haut-Katanga Reproductive Health Programme, members of the Health Zone management teams, and healthcare providers from the selected facilities with at least three years of experience in coordinating and delivering maternal and child health services in Lubumbashi.
Outcome Measures
The major obstetric interventions (MOIs) considered were: caesarean section, hysterectomy, laparotomy for uterine rupture, internal podalic version, craniotomy, and symphysiotomy.
Absolute maternal indications (AMIs) included: haemorrhagic placenta previa, retroplacental haematoma, postpartum haemorrhage, uterine rupture, dystocic presentations, and mechanical dystocia.
The calculation of unmet obstetric needs indicators was based on the following formula:
-
UON or deficit in MOIs for AMIs = (Expected MOIs for AMIs) – (Observed MOIs for AMIs)
-
Observed MOIs for AMIs refer to the number of major obstetric interventions performed for absolute maternal indications during the study period within the target population.
-
Expected MOIs for AMIs were calculated as: Expected births × Reference rate
Expected births during the study period were estimated at 4% of the total population (based on the national vaccination programme in the Democratic Republic of the Congo), and a reference rate of 1.4% was applied, as commonly used in studies within the Unmet Obstetric Needs Network.
Ethical Considerations
This study received ethical approval from the Ethics Committee of the University of Lubumbashi (Approval No. UNILU/CEM/019/2023). Free and informed consent was obtained from all participants. Data confidentiality was ensured through the anonymisation and coding of patients’ medical record numbers.
Results
Socio-demographic characteristics of the study participants
Among the 444 women included in the study, 76% were married. The majority of participants resided in Lubumbashi municipality (35.4%) and the Kenya municipality (13.3%), reflecting the geographical location of the study health facilities, which were predominantly situated in these two areas. Secondary-level education was completed by 53.4% of participants, and the majority of participants were housewives without a specific occupation.
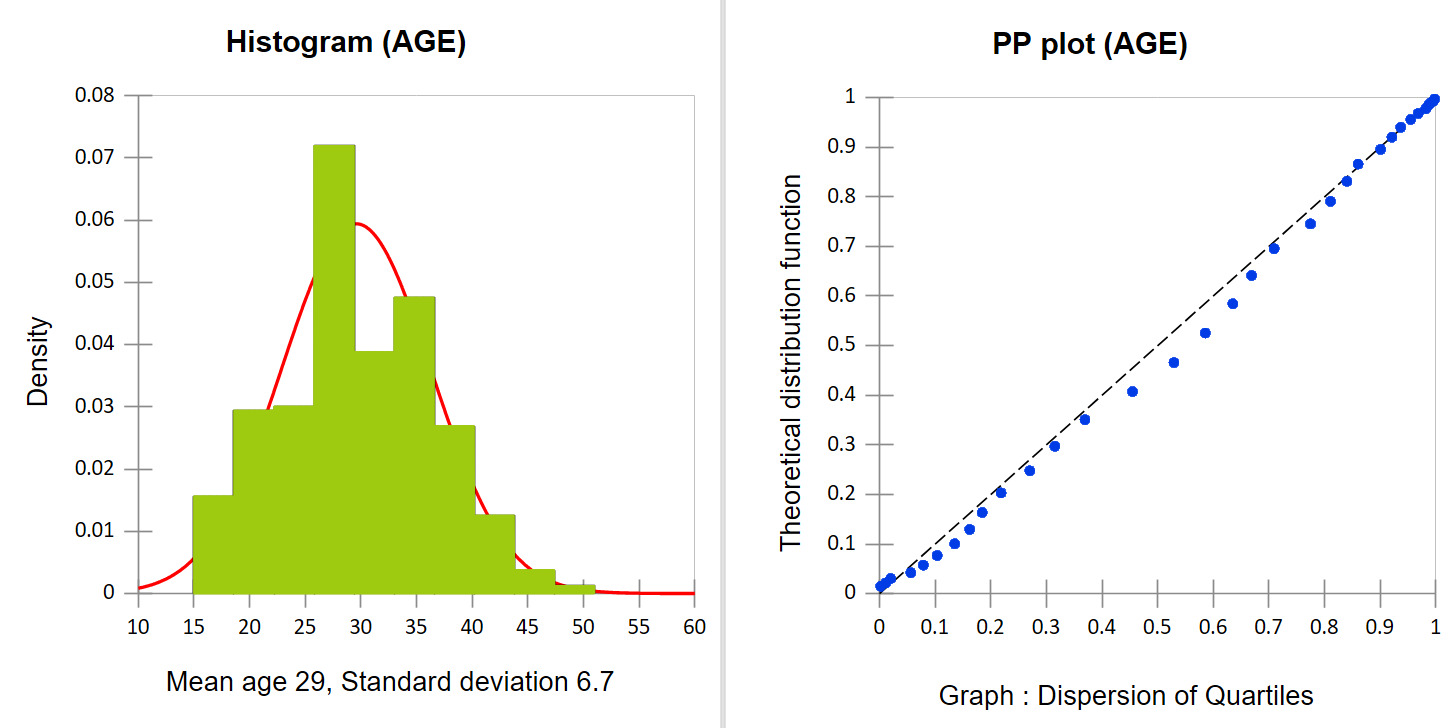
Age of the participants
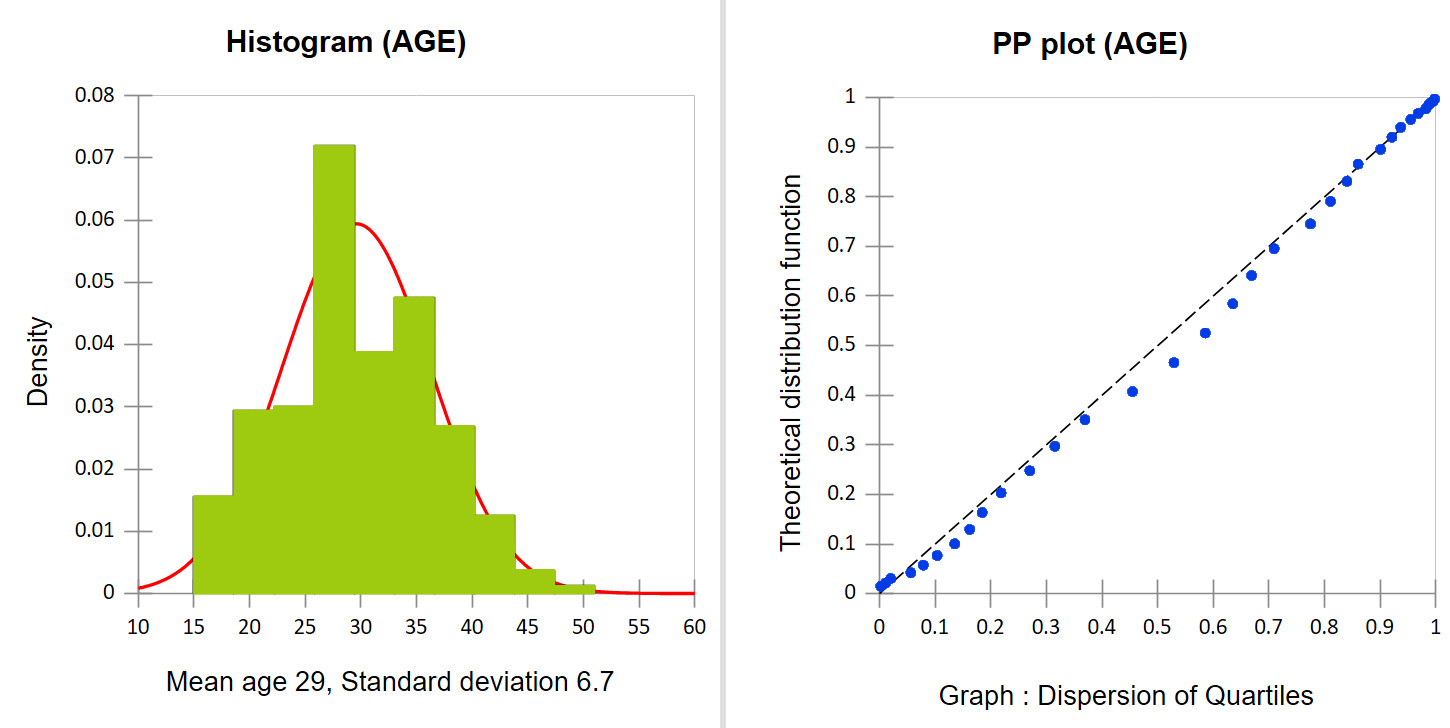
The mean age of women admitted for absolute maternal indications was 29.5 ± 6.7 years. The most common age group was 26–36 years (56.9%). In contrast, Bintou Augusta reported a predominant age group of 20-24 years in Burkina Faso, while Hunger C et al. reported a mean age of 24.5 ± 6.8 years in Tanzania.5–11
Major Obstetric Interventions for Maternal Indications
Uterine rupture was the most frequently reported absolute maternal indication (31.5%), followed by postpartum haemorrhage (17%) and contracted pelvis (16.6%). Caesarean section was the most frequently performed major obstetric intervention in the health facilities included in this study.
Deficits in Major Obstetric Interventions for Absolute Maternal Indications
MOIs – Major Obstetric Interventions and AMIs–Absolute Maternal Indications
In the city of Lubumbashi, the average deficit in major obstetric interventions for absolute maternal indications was 88%. These deficits were higher in secondary-level health facilities, particularly general referral hospitals, with an overall average of 93% across the ten referral facilities, compared with the two tertiary-level facilities, where the deficit was 1% at the University Clinics of Lubumbashi (UCL) and 33% at Sendwe Provincial General Hospital.
Maternal Mortality and Major Obstetric Interventions
MOIs – Major Obstetric Interventions
The overall maternal mortality rate across the twelve study hospitals following a major obstetric intervention was 15.8%. Haemorrhagic shock was the most frequently reported cause of maternal death, accounting for 79% of cases. The most deaths occurred during the postpartum period with 65%. Maternal mortality was highest following caesarean section (17.1%) and hysterectomy (16.6%).
Factors Associated with Maternal Mortality
Multivariate analysis showed that caesarean section was associated with maternal mortality (aOR=1.42; 95% CI:1.21-1.72). In terms of the provision and organisation of care, blood transfusion and referral to a higher level of care were associated with lower odds of maternal death, with risks below 1 among patients who received a blood transfusion or were referred for improved clinical management.
Level of Stakeholders’ Knowledge of the UON Approach
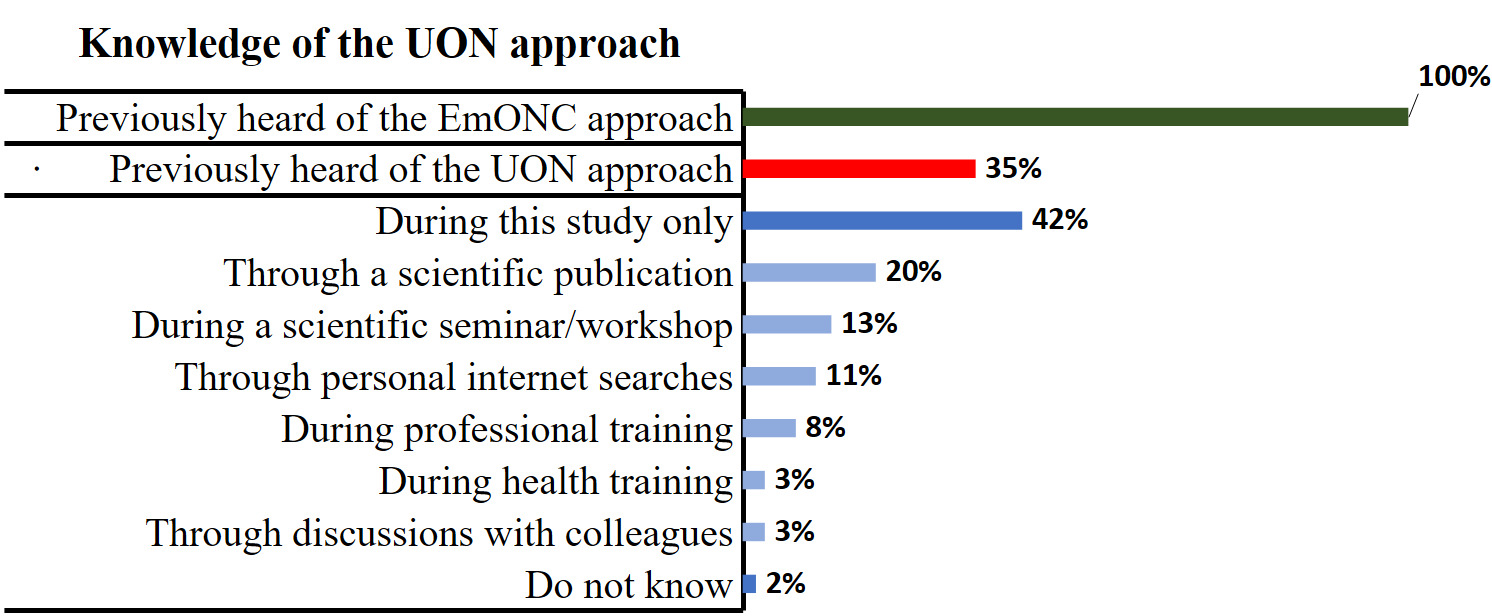
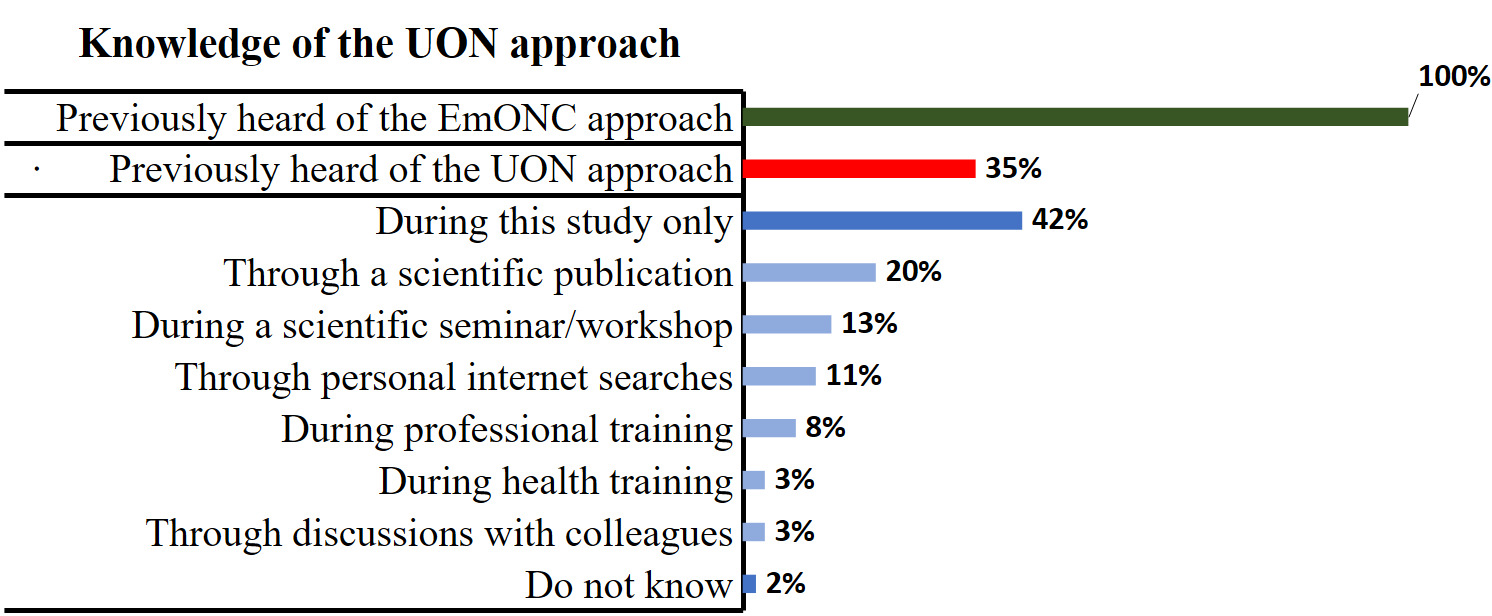
Only 35% of the healthcare providers interviewed had previously heard of the Unmet Obstetric Needs (UON) approach, compared with the Emergency Obstetric and Neonatal Care (EmONC) approach, which was known by 100% of respondents. However, 42% of participants reported that they became aware of the UON approach only during this study.
Discussions
Major Obstetric Interventions for Maternal Indications
Analysis of the types of major obstetric interventions revealed that uterine rupture was the most frequently reported absolute maternal indication (31.5%). Dubourg et al. also identified uterine rupture as the leading absolute maternal indication (40%).12 Hochler et al. demonstrated that the risk of uterine rupture increases linearly with maternal age.13 Similarly, Justus Hofmeyr et al. reported that uterine rupture occurs more frequently in low-income countries than in high-income settings.14
Caesarean section was the most commonly performed major obstetric intervention in health facilities in Lubumbashi (71.6%). These findings are consistent with those reported by Hunger et al. in Tanzania, where caesarean section accounted for 91% of major obstetric interventions in Mtwara.11 Bintou Augusta reported that 80% of major obstetric interventions in the Centre-East health region of Burkina Faso were caesarean sections.5 Likewise, Elizabeth et al. found that more than 90% of major obstetric interventions in Kenya were caesarean sections.15 Our findings are also comparable to those from six studies conducted by the UON Network, where caesarean section accounted for 73% of interventions in Burkina Faso and 98% in Pakistan.16
In this setting, caesarean section remains an effective intervention for reducing unmet obstetric needs and maternal mortality. It plays a crucial role in obstetric practice, particularly in emergency settings.17
Coverage of Deficits in MOIs for AMIs in the City of Lubumbashi
This study identified an average deficit of 88% in major obstetric interventions for absolute maternal indications in the city of Lubumbashi. These findings are comparable to those reported by Bintou Augusta in Burkina Faso, who also observed an average MOI/AMI deficit of 85.31%.5
However, our results differ from those of the UON Network comparative study conducted in urban areas across seven countries, which reported total MOI deficits for AMIs of 26.4% in Benin, 78.6% in Burkina Faso, 64.1% in Haiti, 61.3% in Mali, 60.1% in Morocco, 83.5% in Niger, and 44.5% in Pakistan.16 According to Dubourg et al., improvements in overall access to healthcare services contributed to a reduction in the MOI/AMI deficit in Niger from 83.6% to 70.6% in 2007.1
When disaggregated, unmet obstetric needs deficits across health facilities in the city of Lubumbashi were found to be higher in secondary-level facilities compared with the two tertiary-level institutions, namely the University Clinics and Sendwe Provincial General Hospital. The deficit observed in tertiary facilities is comparable to the reference rate of 1.2% reported in Morocco by De Brouwere et al..3 It is also consistent with rates observed among urban women in Kasongo, DRC (1.1% in 1984), and in Kenya (1.25% in 2008 and 1.3% in 2009) as reported by Elizabeth et al..18
The relatively low deficits observed in tertiary-level facilities may be explained by the quality of obstetric care provided to women admitted with absolute maternal indications, often managed by specialists. In addition, many women admitted to these facilities had attained education beyond secondary level, which may reflect greater awareness of pregnancy-related risks.
In contrast, the higher deficits observed in general referral hospitals in Lubumbashi appear similar to those reported by Mukuna et al., in their study on unmet obstetric needs for major obstetric interventions in three general referral hospitals in the Lomami health division.19 Dubourg et al. in their 2008 study conducted in Senegal, suggested that deficits in major obstetric interventions for absolute maternal indications contributing to maternal deaths were associated with delays in decision-making at the household level to seek care, inadequate antenatal preparation for childbirth and recognition of complications, delays in referral decisions at peripheral facilities, suboptimal emergency management within health facilities, and insufficient preparation of women for transfer.1
Factors Associated with Maternal Mortality
In this study, multivariate analysis demonstrated that the risk of maternal mortality was statistically associated with caesarean section, (aOR=1.42 ; 95% CI:1.21-1.72). This finding is consistent with the study by Kinenkinda et al. on risk factors for maternal and perinatal mortality following caesarean section in Lubumbashi, which reported a significant interaction between the emergency nature of the caesarean indication and maternal mortality, OR=2.18 (95% CI=1.22-3.88).20 Similarly, the meta-analysis by Mascarello et al. indicated that women who underwent caesarean section had a higher risk of maternal death, OR=3.10 (95% CI=1.92-5.00).21
Improving the quality of care and services provided to women undergoing caesarean section can contribute to reducing unmet obstetric needs.17 Analysis of factors related to the provision and organisation of care showed that blood transfusion and referral to tertiary-level facilities were statistically associated with maternal mortality, with risk estimates below 1. This may be explained by the fact that blood transfusion and timely referral to specialised facilities are key pillars in reducing maternal mortality, particularly in cases of postpartum haemorrhage, which remains the leading cause of maternal death. These emergency interventions help correct severe anaemia and restore circulating blood volume, thereby saving lives.
Assessment of Healthcare Providers’ Knowledge of the UON Approach
Knowledge of the UON and EmONC Approaches
Individual interviews revealed limited awareness among healthcare providers regarding the Unmet Obstetric Needs (UON) approach. Approximately half of the respondents reported becoming aware of the UON approach only during the course of this study, in contrast to the Emergency Obstetric and Neonatal Care (EmONC) approach, which was known by nearly all participants. This was illustrated by the following statement from a nurse working in the gynaecology and obstetrics department at Sendwe Provincial General Hospital:
“I have been trained several times in emergency obstetric and neonatal care, and I am familiar with both basic and comprehensive EmONC, but this approach is new to me and I had never heard of it before, even during training at the Health Zone level or here in the department.” (IDI, Nurse, Male, 41 years, Lubumbashi)
Knowledge of the Causes of In-Hospital Maternal Deaths
Half of the interviewees attributed in-hospital maternal deaths to the increasing medicalisation of the health system in Lubumbashi, characterised by the proliferation of private health facilities and the presence of physicians at the primary level of care. In addition, the absence of effective referral and counter-referral mechanisms, as well as financial barriers limiting women’s access to care, were also identified as contributing factors. As highlighted by the administrative manager of the Lubumbashi Health Zone:
“The government aims to move towards universal health coverage, yet the context of Lubumbashi is complex, with a proliferation of private health facilities. While some provide quality obstetric care, many do not and instead retain patients within their facilities without referring women experiencing childbirth complications in a timely manner. When referrals do occur, they are often delayed, possibly to avoid being associated with maternal deaths.” (IDI, Health Zone Administrator, Male, 53 years, Lubumbashi)
Strengths and Limitations
The first limitation of this study relates to its external validity, due to differences in the quality of obstetric care across the selected health facilities, particularly regarding the availability of qualified personnel, technical capacity, and variations in the epidemiological profiles of service users.
The second limitation relates to methodological challenges in applying the unmet obstetric needs concept, which remains relatively unfamiliar within the professional context. The selection of the reference rate is a critical element in UON studies. Owing to deficiencies in data reporting and archiving systems, a reference rate of 1.4%, as used in UON Network studies, was adopted.
Finally, the retrospective nature of the data collection, rather than a prospective approach, constituted an additional limitation of this study.
Conclusions
This study highlights a substantial burden of unmet obstetric needs in the city of Lubumbashi, reflected by a high overall deficit in major obstetric interventions for absolute maternal indications, particularly within secondary-level health facilities. In contrast, tertiary-level institutions demonstrated comparatively lower deficits, suggesting better availability and quality of specialised obstetric care. The findings also underscore the persistence of maternal mortality following major obstetric interventions, with haemorrhagic complications remaining the leading cause of death. Caesarean section was statistically associated with maternal mortality risk, while access to blood transfusion and timely referral to higher levels of care appeared to play a protective role, highlighting the importance of functional referral systems and emergency response capacity.
Beyond service delivery gaps, the study revealed limited awareness among healthcare providers regarding the Unmet Obstetric Needs (UON) approach, despite widespread familiarity with Emergency Obstetric and Neonatal Care (EmONC). This knowledge gap may hinder the effective integration of UON indicators into routine planning and performance monitoring. Strengthening provider awareness, improving access to life-saving interventions at secondary-level facilities, and reinforcing referral mechanisms are essential for reducing unmet obstetric needs and maternal mortality. The UON indicator therefore represents a valuable tool for assessing health system performance and guiding targeted interventions aimed at improving equitable access to quality obstetric care in resource-constrained urban settings.
Strengthening emergency obstetric care capacity at secondary-level facilities, improving referral systems, and integrating UON indicators into routine health information systems should be prioritized to reduce preventable maternal deaths.
Abbreviations
UON: Unmet Obstetric Needs; UCL: University Clinics of Lubumbashi, DHIS: District Health Information System; AMI: Absolute Maternal Indication, MOI: Major Obstetric Intervention MICS: Multiple Indicator Cluster Surveys; ODK: Open Data Kit; QGIS: Quantum Geographic Information System; DRC: Democratic Republic of Congo; SNCC: National Railway Company of the Congo; NHIS: National Health Information System; EmONC: Emergency Obstetric and Neonatal Care; SPSS: Statistical Package for the Social Sciences; WHO: World Health Organization.
Acknowledgements
We would like to express our sincere gratitude to the School of Public Health of Lubumbashi, particularly Professors Albert Mwembo Tambwe-A-Nkoy and Paul Makan Mawaw, for their guidance and valuable technical support throughout this work. We also extend our appreciation to the Institute of Tropical Medicine in Antwerp, through Professor Déogratias Katsuval Sibongwere, for funding part of this research. We are equally grateful to Professors Abel Ntambue and Ngashi Ngongo for their contributions. Our sincere thanks also go to the Ethics Committee of the University of Lubumbashi and to the entire coordination team of the School of Public Health of Lubumbashi.
Ethics statement
This study received ethical approval from the Ethics Committee of the University of Lubumbashi (Approval No. UNILU/CEM/019/2023). Free and informed consent was obtained from all participants. Data confidentiality was ensured through the anonymisation and coding of patients’ medical record numbers.
Data availability
The datasets generated and/or analyzed during this study are available from the corresponding author upon reasonable request.
Funding
Part of this research was supported through a financial agreement between the School of Public Health of Lubumbashi and the Institute of Tropical Medicine in Antwerp, within the framework of support for the Master of Public Health programme. The article publication charge (APC) was not funded by any organization.
Authorship contributions
All authors read and approved the final version of the manuscript. Christian Baboko conceived the study and its design, formulated the research question, conducted both the quantitative and qualitative analyses, prepared the results, drafted the manuscript, and incorporated co-authors’ comments into the final version. Albert Mwembo Tambwe contributed to the study design, coordination, and supervision. Paul Makan Mawaw participated in the study design and oversaw the planning and implementation of research activities. Deogratias Katsuva contributed to resource mobilisation to support data collection. Ngashi Ngongo provided supervision in impact modelling using the LiST tool. Abel Ntambue supervised the mixed-methods research methodology. Louis Sumba provided guidance on the statistical analyses. Emerite Disuemi, Angel Alworonga, and Gertrude Mapele contributed to quantitative data collection. All authors approved the final manuscript prior to submission.
Disclosure of interest
The authors completed the ICMJE Disclosure of Interest Form (available upon request from the corresponding author) and disclose no relevant interests.
Corresponding Author
Name Surname: Baboko Ilako Christian, MD, MPH
Institution: School of Public Health, University of Lubumbashi,
Address: 1 Bongolo Road, Kalamu, Kinshasa-DRC
Country: Democratic Republic of Congo
Contacts: +243 817 607 573/ +243 990 236 335
Email: <Baboko.Ilako@Unilu.ac.cd/> c.babokoilako@who.int