Cardiovascular disease is the leading cause of death and disability worldwide, affecting more than 500 million individuals and accounting for an estimated 18.6 million deaths in 2019, with a disproportionately high burden in low- and middle-income countries.1,2 While the epidemiology of cardiovascular disease in older age groups is well characterized, it remains relatively understudied in younger populations. A recent global analysis reported modest declines in cardiovascular disease mortality alongside rising prevalence among individuals aged 15-39 years.3 However, aggregating this broad age range may obscure important life-stage differences, particularly among young adults aged 20-24 years.
Young adulthood represents a distinct transitional period characterized by exit from pediatric and adolescent health systems, entry into higher education or the workforce, and increasing autonomy over health behaviors such as diet, physical activity, and substance use. This developmental stage is often accompanied by changes in lifestyle behaviors and metabolic risk factors that shape long-term cardiovascular risk trajectories. Broader age groupings, such as 15-24 or 20-29 years, encompass heterogeneous developmental, social, and healthcare contexts and may therefore mask early adult-specific patterns of cardiovascular burden.
The impact of cardiovascular disease in young adults is likely to be greater in low- and middle-income countries due to younger population structures, rising cardiometabolic risk factor burdens, limited access to preventive and primary care services, and greater downstream economic consequences. The Global Burden of Disease framework provides standardized and comparable estimates across countries and over time, making it uniquely suited for assessing global and regional cardiovascular disease burden in young adult populations. Accordingly, in this study we analyzed Global Burden of Disease 2021 data among individuals aged 20-24 years from 1990-2021, examining global trends stratified by Sociodemographic Index (SDI) quintiles and evaluating the relative contributions of behavioral, metabolic, and environmental risk factors to cardiovascular disease burden in this age group.
METHODS
We analyzed data from the Global Burden of Disease Study 2021, an international initiative led by the Institute for Health Metrics and Evaluation. The Global Burden of Disease study uses standardized case definitions and Bayesian meta-regression and ensemble modeling to generate consistent, age-standardized estimates of disease burden across 204 countries and territories.4 Estimates are periodically updated using standardized methodologies, with back-casting applied to ensure internal consistency over time despite updates to data sources and modeling approaches.
Using the publicly accessible Global Burden of Disease Results Tool, we extracted annual estimates from 1990-2021 for individuals aged 20-24 years for the cause group “cardiovascular diseases.” We obtained both age-standardized rates (per 100,000 population) and absolute counts for prevalence, deaths, and disability-adjusted life years, disaggregated at the global level and by Sociodemographic Index quintiles (low, low-middle, middle, high-middle, and high).4 We further extracted disability-adjusted life year rates attributable to individual risk factors, grouped into three broad categories: behavioral, metabolic, and environmental or occupational.
Temporal trends in disability-adjusted life year rates by risk factor from 1990-2021 were visualized using annual age-standardized estimates. All analyses and figures were generated in R (version 4.3.2; R Foundation for Statistical Computing).
RESULTS
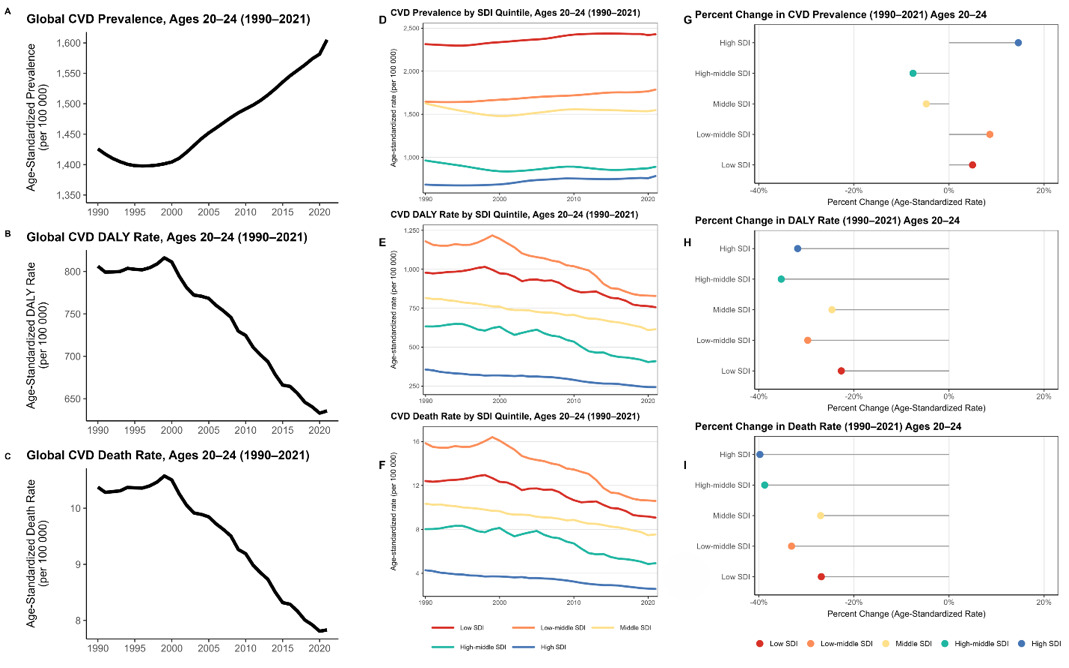
From 1990-2021, the global number of individuals aged 20-24 years living with cardiovascular disease increased from 7.0 to 9.6 million (+37%), with the age-standardized prevalence rate increasing by 12.6% (95% uncertainty interval=9.7-15.5%), from 1,426 to 1,605 per 100,000 population (Figure 1). In 1990, low- and low-middle-Sociodemographic Index regions accounted for 38% of all global cardiovascular disease cases among individuals aged 20-24 years; by 2021, this proportion had increased to 60%. Low-Sociodemographic Index regions experienced the largest absolute increase, adding 1.55 million cases (+157%), followed by low-middle-Sociodemographic Index regions (1.41 million cases, +82%). In contrast, middle-Sociodemographic Index regions showed a modest decline (-5%), high-middle-Sociodemographic Index regions experienced the steepest proportional decrease (-29%), and high-Sociodemographic Index regions showed a modest increase (+9%).
__1990-2021__prevalence__dalys__deaths__and_.png)
Globally, the age-standardized disability-adjusted life year rate declined from 806 to 636 per 100,000 population (-21%), while the age-standardized death rate decreased from 10.4 to 7.8 per 100,000 population (-25%). Uncertainty intervals were examined for all estimates, and the direction and magnitude of key trends remained consistent across uncertainty bounds.
As shown in Figure 1, high-Sociodemographic Index regions recorded the largest proportional increase in prevalence (+14.6%; 95% uncertainty interval=4.2-27.9%), accompanied by substantial reductions in disability-adjusted life year and death rates (-31.8% and -39.8%, respectively). Low-Sociodemographic Index regions experienced smaller increases in prevalence (+4.9%) alongside more modest declines in disability-adjusted life year and death rates (-22.7% and -26.9%). In contrast, middle- and high-middle-Sociodemographic Index regions demonstrated decreases in prevalence (-4.8% and -7.6%), disability-adjusted life year rates (-24.6% and -35.3%), and death rates (-27.0% and -38.8%). Overall, these findings indicate divergent Sociodemographic Index–specific trajectories, with rising prevalence but marked reductions in severe outcomes in high-Sociodemographic Index regions, compared with increasing case counts and slower improvements in disability-adjusted life years and mortality in lower-Sociodemographic Index settings.
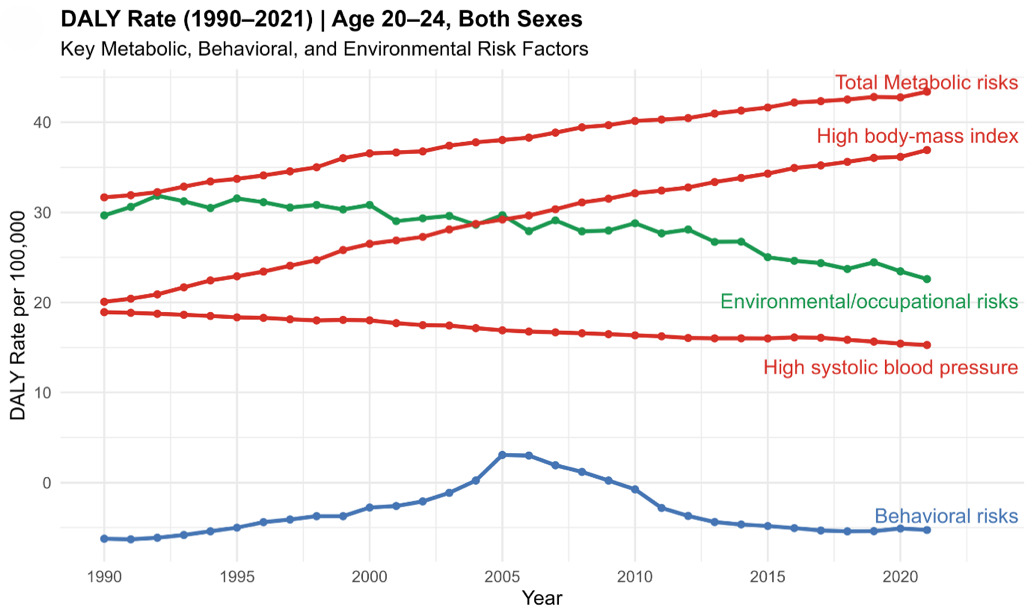
Across all risk categories, metabolic exposures accounted for the largest share of cardiovascular disease disability-adjusted life year burden in this age group (Figure 2). From 1990-2021, disability-adjusted life year rates attributable to high body-mass index increased by 89.8%, while total metabolic risk–attributable disability-adjusted life years increased by 44.7%. In contrast, disability-adjusted life year rates attributable to high systolic blood pressure declined by 14.0%. Environmental or occupational risk–attributable disability-adjusted life years decreased by 21.3%, and behavioral risk–attributable disability-adjusted life years decreased by 5.5%, indicating slower progress in modifying behavioral exposures compared with metabolic risk factors during early adulthood.
_rates_attributable_to_behavioral.png)
DISCUSSION
Our findings are consistent with prior Global Burden of Disease analyses demonstrating reductions in age-standardized disability-adjusted life years and mortality among younger populations, alongside persistent increases in prevalence across most regions.2,3 Specifically, the 2019 Global Burden of Disease analysis reported a 21% reduction in age-standardized disability-adjusted life years and a 15% reduction in mortality between 1990 and 2019 among individuals aged 15-39 years.2 By disaggregating this broad age range, our study extends existing evidence by quantifying absolute prevalence increases specifically among young adults aged 20-24 years. Notably, we observed a 22 percentage-point shift in absolute cardiovascular disease cases toward low- and low-middle-Sociodemographic Index regions over three decades, highlighting early-established and widening geographic inequities in young adult cardiovascular burden.
This shift likely reflects a convergence of demographic, structural, and health system factors. Low- and low-middle-Sociodemographic Index regions are experiencing rapid growth in young adult populations, rising exposure to metabolic risk factors, and uneven access to preventive and primary care services. Limited screening, delayed diagnosis, and constrained healthcare capacity may contribute to higher disease burden and slower declines in disability-adjusted life years and mortality compared with high-Sociodemographic Index settings. In contrast, high-Sociodemographic Index regions may exhibit rising prevalence alongside declining disability-adjusted life year and death rates due to improved survival, earlier detection, and more effective long-term disease management. This pattern is consistent with an epidemiologic transition from fatal to chronic cardiovascular disease burden in early adulthood and suggests that improvements in diagnosis and survival, rather than true reductions in disease occurrence, may underlie the observed divergence between prevalence and severe outcomes across Sociodemographic Index contexts.
Recent evidence from the NCD Risk Factor Collaboration indicates that increases in hypertension and obesity from 1990-2022 have been greatest among young adults, particularly in the Pacific Islands, the Middle East and North Africa, and South Asia.5,6 These regions also demonstrated the most rapid growth in cardiovascular disease–related disability-adjusted life years in our analysis. Taken together, these findings highlight the central role of structural and socioeconomic determinants, beyond individual-level risk factors alone, in shaping early-life cardiovascular risk across Sociodemographic Index settings.
Our findings should be interpreted in the context of several limitations. First, Global Burden of Disease estimates rely on modeled data derived from heterogeneous sources, and limited primary surveillance data in low-Sociodemographic Index regions necessitate greater reliance on statistical modeling and imputation, which may introduce additional uncertainty. Although uncertainty intervals are incorporated within the Global Burden of Disease framework, estimates from data-sparse settings should be interpreted as population-level patterns rather than precise point estimates. Second, outcomes were not disaggregated by sex or by specific cardiovascular disease subtypes, potentially masking important heterogeneity in early-life cardiovascular risk profiles. Third, risk attribution was limited to exposures included within the Global Burden of Disease framework and may not fully capture age-relevant or emerging risk factors among young adults, such as conflict exposure, displacement, or evolving behaviors including e-cigarette use and energy drink consumption. Finally, temporal changes in reporting practices and measurement error may influence observed trends, particularly for behavioral risk factors, underscoring the need for caution when translating global estimates into policy, especially in data-sparse settings.
CONCLUSIONS
Our findings demonstrate an increase in the prevalence and burden of cardiovascular disease among young adults aged 20-24 years from 1990-2021, with a marked shift toward low- and low-middle-Sociodemographic Index regions and worsening metabolic risk profiles, particularly elevated body-mass index, as key contributors. This age group represents a critical window for early-life cardiovascular prevention, with substantial potential to alter long-term cardiovascular risk trajectories and reduce future disease burden.
Policy strategies such as sugar-sweetened beverage taxation, trans-fat elimination, and dietary guidelines aligned with World Health Organization recommendations may help mitigate worsening metabolic risk when implemented early in the life course, particularly in low-resource settings. However, the feasibility, cost-effectiveness, and clinical utility of specific interventions were not evaluated in this study and warrant further investigation.
Persistent environmental and occupational exposures, including fine particulate matter (PM2.5), highlight the importance of structural and regulatory approaches to address upstream determinants of cardiovascular risk.7 Clinically, early identification and risk assessment during young adulthood may offer an important opportunity for prevention, although optimal screening strategies remain to be defined. Future research should prioritize age-specific surveillance and intervention studies to inform targeted prevention strategies during early adulthood.
Acknowledgements
Portions of this study will be presented at the American Public Health Association (APHA) 2025 Annual Meeting and Expo on November 3, 2025.
Disclaimer
None.
Ethics statement
This study used publicly available and de-identified data and was exempt from institutional review board approval.
Data availability
The data used in this study are publicly accessible from the Global Burden of Disease Study 2021 via the Institute for Health Metrics and Evaluation Global Burden of Disease Results Tool.
Funding
This research received no specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Authorship contributions
AN contributed to study conception and manuscript writing. JA contributed to data analysis and manuscript writing. PP and EM contributed to critical revision of the manuscript. SAK contributed to study design, supervision, and critical revision. All authors approved the final manuscript.
Disclosure of interest
The authors completed the ICMJE Disclosure of Interest Form (available upon request from the corresponding author) and disclose no relevant interests.
Correspondence to
Sadeer Al-Kindi
Center for Cardiovascular Computational and Precision Health (C3PH)
Department of Cardiology, Houston Methodist
Houston, Texas, United States of America
sal-kindi@houstonmethodist.org