Antenatal care (ANC) is defined as the set of interventions that ensure optimal care for pregnant women, thereby reducing maternal and neonatal risks.1 It encompasses several dimensions, including provider qualifications, infrastructure and equipment, and access to clinical and paraclinical examinations. Effective ANC involves early pregnancy monitoring, screening for complications, raising awareness of maternal health practices, and administering preventive treatments such as iron and folic acid supplements.2
Provider qualifications and the use of appropriate diagnostic tools are crucial for improving ANC, significantly reducing maternal and neonatal morbidity and mortality.3 Conversely, ineffective services are often linked to unattended deliveries and elevated maternal mortality.4 Governance and regulation of medical practices also shape ANC quality, with structured organization of services being essential.5 Evidence from Mali shows that 70% of consultations were conducted by midwives, 10% by obstetric nurses, and 20% by traditional birth attendants, underscoring the impact of provider qualifications.1,2 Yet, shortages of skilled personnel remain a major obstacle in resource-limited countries.6 In Senegal, only half of midwifery staffing needs are met, creating significant service gaps.5
Infrastructure and equipment further influence ANC effectiveness. In Côte d’Ivoire, deficiencies prevented providers from performing essential procedures, increasing nosocomial infection risks.7 In Nyarambe, similar shortcomings contribute to persistently high maternal mortality despite ANC coverage reaching 90% in 2022.8
Recognizing these disparities, WHO and the United Nations have set ambitious targets to strengthen prenatal care through better management of equipment and human resources.9 In conflict-affected regions such as Nyarambe, insecurity exacerbates these challenges by disrupting supply chains, limiting supervision, and driving staff turnover.
A thorough evaluation of ANC services in Nyarambe is therefore essential to identify determinants of care quality and propose targeted interventions. The aim of this study is to determine the proportion of facilities offering quality ANC and to identify factors associated with ANC service quality in maternity units within the Nyarambe Health Zone.
II. METHODS
1. TYPE OF STUDY
This analytical cross-sectional study was conducted in the Nyarambe Health Zone, located in Ituri Province, Democratic Republic of Congo (DRC), from March 4, 2025 to March 30, 2025.
2. STUDY FRAMEWORK
The Nyarambe health zone is one of 36 health zones in the Ituri provincial division. It is located in the northeast of the DRC, an area plagued by armed conflict that exacerbates the already precarious situation of the population. The zone has a population of 284,321 inhabitants. The main sources of income are artisanal fishing, livestock farming (both large and small), subsistence agriculture, and small-scale trade. It comprises 23 health centers and one general referral hospital (HGR).
3. SAMPLING
Study Population and Selection Criteria
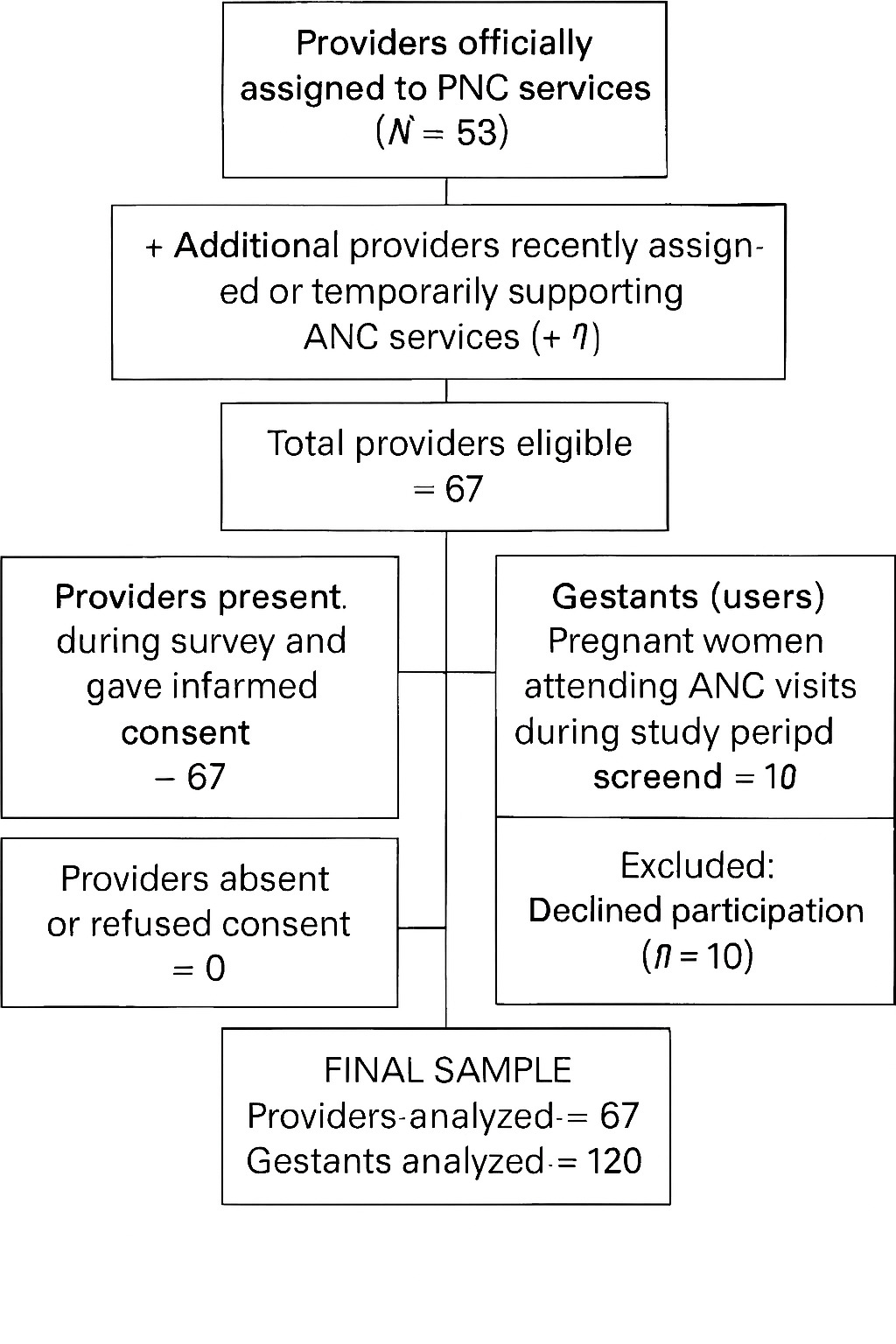
The study included ANC providers in all health facilities and pregnant women attending ANC visits. Eligible participants were authorized staff and consenting gestants; exclusions were absent staff or refusal to consent. Women’s perspectives on satisfaction, respect, waiting time, information, and access barriers were captured
Sample Size
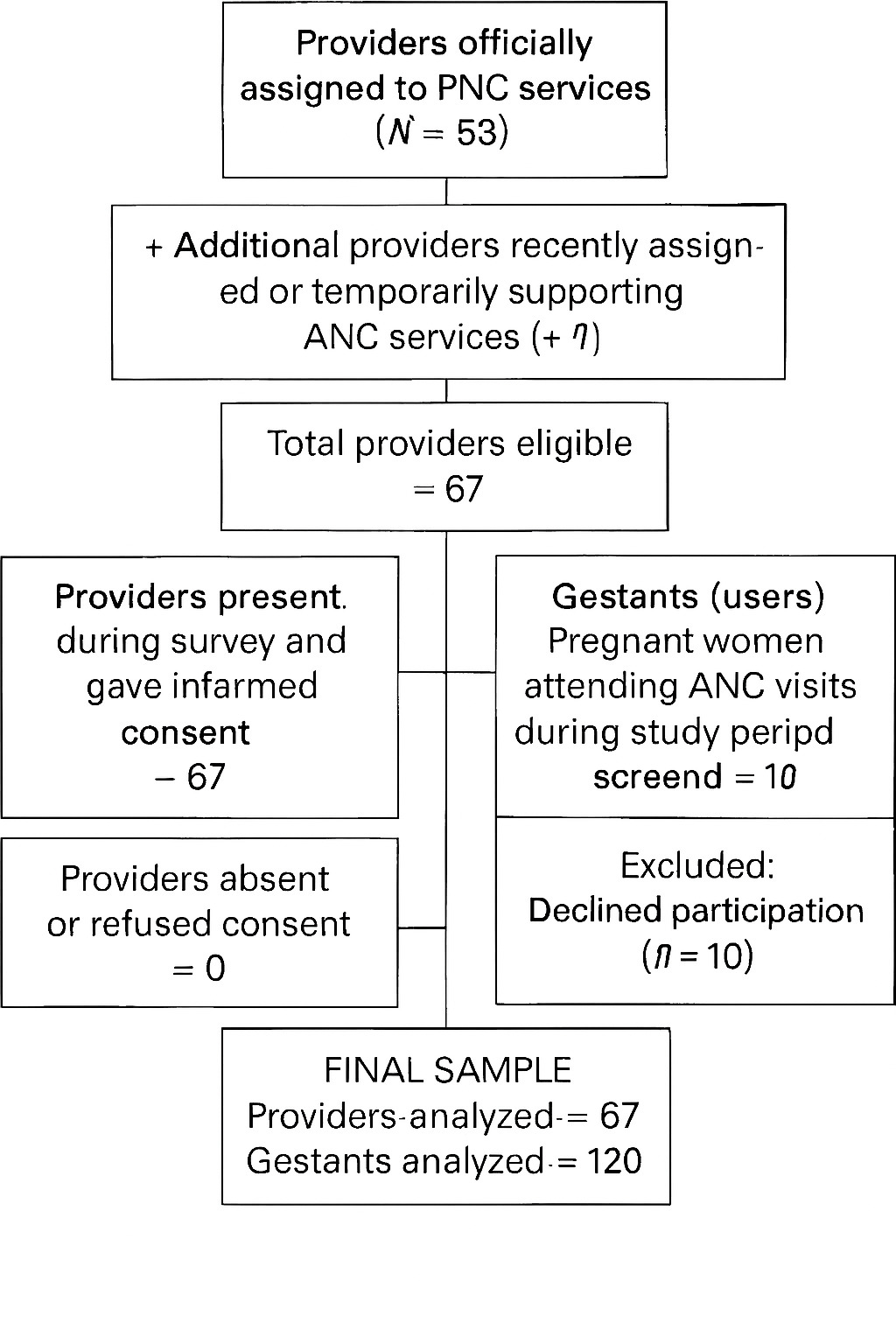
A total of 67 providers were included in the study, despite a larger number being officially assigned to ANC services. This discrepancy reflected recent staff assignments, inclusion of both hospital- and health center-based providers, and temporary recruitment to support ANC. The minimum sample size was estimated at 49 using the Epi Info 7 finite population formula ( n=N⋅Z²⋅p(1−p)d²(N−1)+Z2⋅p(1−p) with Z=1.96, d=0.05, p=0.5). To account for clustering across 23 health centers and one general referral hospital (HGR), a design effect of 1.23 was applied, with an additional 10% for nonresponses, yielding a final target of 67 providers. All eligible staff were exhaustively included to maximize representativeness. For gestants, a convenience sample of 120 women was recruited proportionally across facilities, ensuring perspectives from both hospital and health center users
Sampling Technique
-
Providers: Exhaustive inclusion of all staff assigned to ANC services across the 23 health areas and the HGR.
-
Gestants : Consecutive sampling of ANC attendees during the study period.
To reduce bias, stratification was applied by facility type (health centers vs. HGR), and results were adjusted for clustering at the facility level.
4. STUDY VARIABLES
-
Dependent variable: Quality of antenatal care (ANC), constructed from two components:
-
Inputs: personnel, equipment, medications, infrastructure.
-
Process: interview, physical examination, paraclinical tests, preventive care.
-
-
Independent variables: provider characteristics (age, education, seniority, training, supervision), facility type, and user-reported satisfaction indicators.
5. DATA COLLECTION
Data collection employed complementary methods to enhance robustness: structured provider interviews using Kobocollect, direct non-participant observations of ANC visits, exit interviews with gestants to assess satisfaction, respect, waiting time, information received, and barriers to access, plus systematic reviews of ANC records and registers for triangulation. Indicators were adapted from validated frameworks (WHO/UNICEF SARA, DHS SPA, ANC content indices), and observers followed uniform protocols. Internal consistency of the composite quality score was verified with Cronbach’s alpha. A pragmatic threshold of 60% was set to define good quality, consistent with local benchmarks. To reduce the Hawthorne effect, observations were unannounced and repeated, with findings cross-checked against registers and patient reports. Limitations included reliance on a convenience threshold, lack of explicit modeling of facility type, and absence of formal inter-observer reliability testing. Nonetheless, investigators were uniformly trained, and a pretest minimized discrepancies
6. DATA ANALYSIS
Data were collected via KoboCollect and exported to SPSS v25.0, with descriptive statistics generated in SPSS and Excel. Qualitative variables were summarized as proportions and frequencies, while quantitative variables were expressed as means ± standard deviations or medians with interquartile ranges, depending on distribution verified by the Kolmogorov-Smirnov test.
A composite quality score was constructed by binary coding each indicator (1 = present, 0 = absent), summing, and converting into percentages. Scores ≥80% were classified as “good quality,” 60–79% as “satisfactory,” and <60% as “unsatisfactory.” For regression analysis, “good” and “satisfactory” were grouped as “acceptable quality” (coded 1), while “unsatisfactory” was coded 0. This threshold, based on local benchmarks, provided a pragmatic distinction between acceptable and poor ANC services, though not formally validated.
Statistical modeling followed a structured approach: bivariate logistic regression identified crude associations, multivariate regression adjusted for confounders, and mixed-effects regression accounted for clustering of providers within facilities. Results were reported as odds ratios (OR/aOR) with 95% confidence intervals, using a 5% significance level. Collinearity was assessed with variance inflation factors (VIFs), applying corrective strategies when necessary.
7. ETHICAL CONSIDERATIONS
Approval was obtained from the Ethics Committee of the Kinshasa School of Public Health (ESPK), reference ESP/CE/51/2025. Informed consent was obtained from all participants (providers and gestants). Confidentiality and anonymity were guaranteed. Administrative authorization was granted by local health authorities, and community permission was secured through local leaders and health committees
III. RESULTS
3.1. SOCIODEMOGRAPHIC CHARACTERISTICS OF SERVICE PROVIDERS
Among the 67 prenatal care providers surveyed, the majority were women (94%). Ages ranged from 23 to 68 years, with a mean age of 44. In terms of education, 50.7% held an A1/A2 diploma, while more than half (53.7%) were registered nurses. Professional experience was substantial, with 74.6% having more than five years of practice compared to 25.4% with less than five years (Table I).
3.2. QUALITY OF ANTENATAL CARE (ANC) IN HEALTH FACILITIES
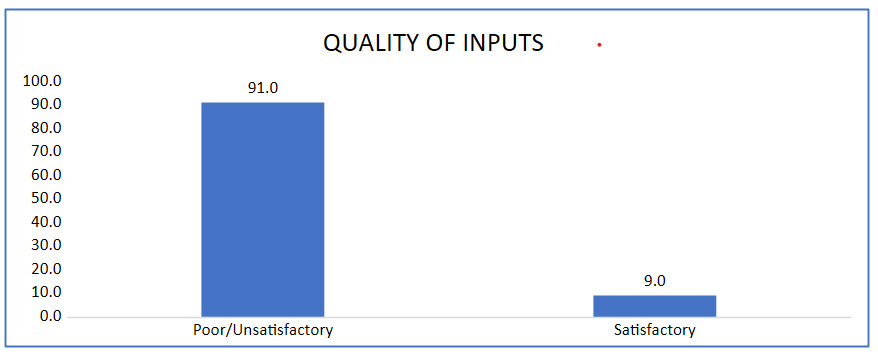
3.2.1. QUALITY OF INPUTS
Inputs across human resources, infrastructure, equipment, and medications were largely inadequate, with 91% reporting poor conditions. Consultation spaces (88.1%) and reception rooms (61.2%) were common, but family planning (0%), counseling (4.5%), and sample collection rooms (9%) were scarce. Basic tools like basins (83.6%) and thermometers (71.6%) were available, while ultrasound (6%) and CD4 counters (0%) were absent. ANC registries (98.5%) and cards (95.5%) were accessible, but referral slips (59.7%) and lab forms were limited. Medications such as Fansidar (98.5%) and antibiotics (97%) were adequate, yet HIV (20.9%) and syphilis tests (26.9%) were critically lacking.
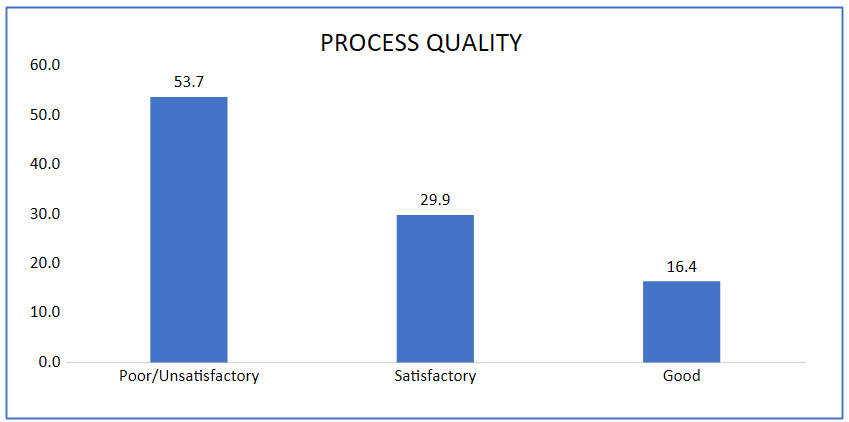
3.2.2. QUALITY OF PROCESSES
Process quality was also unsatisfactory. Interviews covered general symptoms (76.1%), headaches or blurred vision (71.6%), edema (68.7%), and vaginal bleeding (61.2%), but respiratory symptoms were rarely addressed (28.4%). Physical examinations were more consistent: fundal height and fetal heart sound assessments were performed universally (100%), weight was measured in 92.5%, anemia checks in 73.1%, and edema testing in 71.6%. Lymph node examinations were infrequent (25.4%). Diagnostic testing was notably weak, with HIV (26.9%) and syphilis (19.4%) being the most common, while blood typing (10.4%), hemoglobin (9.0%), glucose and urine tests (6.0%), and toxoplasmosis (4.5%) were rarely performed.
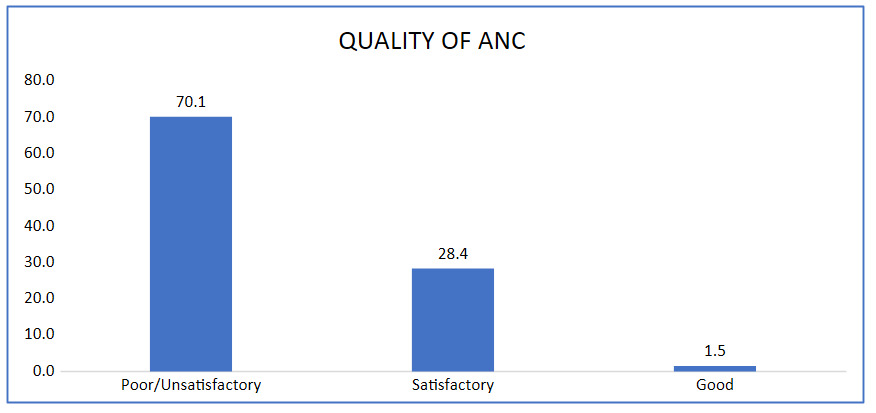
3.2.3. OVERALL QUALITY OF ANC
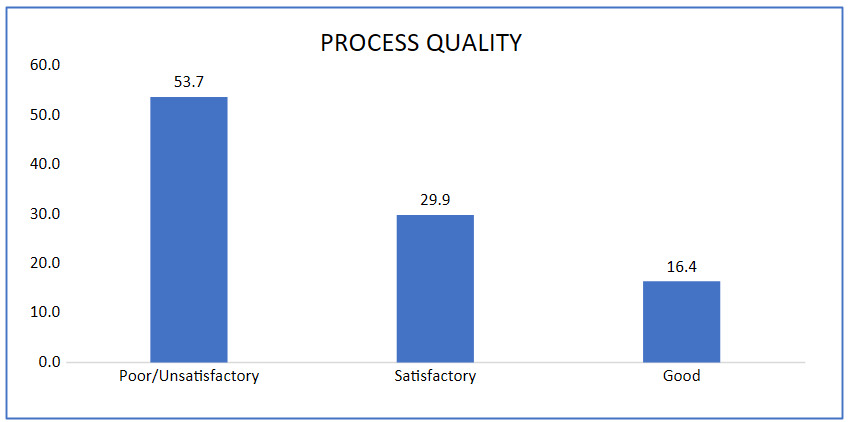
When combining inputs and processes, overall quality was insufficient. A majority (70.1%) of respondents rated services as poor or unsatisfactory, while only 28.4% considered them satisfactory. Using the recoded threshold (≥60% = acceptable, <60% = unacceptable), more than two-thirds of facilities fell into the unacceptable category (Figure 4).
_i.png)
_in_health_facilities_in_the_nya.png)
3.3. FACTORS ASSOCIATED WITH QUALITY OF ANC
The logistic regression highlights several key associations with ANC quality. Training received significantly improves outcomes, with adjusted odds showing a protective effect (ORa=0.58, p=0.012). Lack of diagnostic tests increases the risk of poor ANC quality both in bivariate (ORb=4.91, p=0.006) and multivariate analysis (ORa=2.14, p=0.014). Availability of basic equipment was significant in bivariate analysis but lost significance after adjustment (p=0.234), suggesting confounding. Drug availability remains a strong predictor, with adjusted results showing better ANC quality when drugs are available (ORa=0.72, p=0.001). Overall, training, diagnostic testing, and drug availability emerge as the most consistent determinants of ANC service quality.
IV. DISCUSSION
QUALITY OF INPUTS
The Prenatal care (PNC) in the Nyarambe Health Zone was judged unsatisfactory in 91% of cases, reflecting critical shortages of human, material, and medicinal resources.10 The absence of essential diagnostic equipment, including CD4 counters (0.0%) and HIV/syphilis screening tests, severely limits early detection of maternal infections and compromises obstetric monitoring.11,12 Infrastructure disparities are evident: while examination rooms are relatively available (88.1%), educational spaces remain under-resourced (37.3%), restricting patient information and awareness.13 Comparable challenges have been documented in Kenya, where inadequate equipment undermines prenatal care,14 and in Mali, where limited access to diagnostic tools (RPR/HIV/CD4 <10%) weakens infection detection.15 These findings highlight a regional issue, though differences in governance and health system organization must be considered when drawing cross-country parallels.
Insecurity in Ituri further exacerbates resource gaps, contributing to stock ruptures, disrupted supply chains, staff turnover, and reduced supervision. These factors weaken quality assurance and interact with provider workload, governance, and facility management. Inadequate training compounds the problem, as shown in the DRC, where 91% of respondents rated care as poor.16 Similarly, in Côte d’Ivoire, high drug availability did not translate into better care when infrastructure and organization were deficient.17 Strengthening human resources, infrastructure, governance, and supply chain resilience is therefore essential, as medication alone cannot ensure effective prenatal care.
QUALITY OF PROCESSES
Process quality in Nyarambe revealed major gaps. While essential examinations such as uterine height measurement and fetal heart sound assessment were consistently performed, screening for maternal infections was inadequate, with HIV (26.9%) and syphilis (19.4%) testing far below recommended standards.18 Limited lymph node checks (25.4%) and scarce toxoplasmosis (4.5%) and hemoglobin (9.0%) tests further hindered early detection of infections and anemia.19 These deficiencies mirror findings from Kenya and Mali, highlighting a regional challenge of poor diagnostic access.14,15
Insecurity worsens these gaps by disrupting laboratory supply chains and discouraging attendance, yet other determinants—provider workload, weak supervision, and poor adherence to protocols—also undermine care. Evidence from Guinea shows similar deficiencies linked not only to insecurity but also to inadequate training and fragmented organization.20 Thus, governance, supervision, and workforce capacity are as critical as security in shaping ANC process quality.
FACTORS ASSOCIATED WITH ANC SERVICE QUALITY
The quality of antenatal care (ANC) in Nyarambe is shaped by provider capacity, institutional resources, and broader systemic conditions. Training emerges as a decisive factor, not only by equipping providers with technical skills but also by reinforcing adherence to updated protocols and strengthening confidence in clinical decision-making. Evidence from Kenya and Mali shows that continuous professional development improves diagnostic accuracy and patient outcomes.2,10
Diagnostic testing is equally critical. Where tests are routinely available, providers can detect complications early and tailor interventions. Conversely, limited access, as seen in parts of Central and West Africa, undermines monitoring and exposes women to preventable risks.3,11,21 Drug availability complements this picture: consistent supplies enable effective care, while shortages perpetuate inequities and erode trust in health systems.
Material resources such as equipment are necessary but insufficient without trained staff and governance structures to ensure proper use and accountability. In Nyarambe, the absence of standardized protocols illustrates how even well-equipped facilities may deliver uneven care.5,18
The security situation in Ituri further complicates service delivery, disrupting supervision, increasing provider workload, and weakening governance. Yet insecurity interacts with systemic weaknesses, poor management, limited oversight, and inadequate training—rather than acting alone. Comparisons with Kenya and Mali highlight shared diagnostic challenges but also emphasize the importance of local governance and cultural contexts.
Improving ANC quality in Nyarambe therefore requires integrated reforms: strengthening supervision, investing in provider training, ensuring reliable diagnostic services, and addressing insecurity to guarantee equitable and effective prenatal care in fragile settings
STRENGTHS AND LIMITATIONS
This study offers valuable insights into ANC quality in Nyarambe, using triangulated data sources and internationally validated frameworks, enhancing robustness and comparability. Strengths include provider perspectives and a pragmatic composite quality score, though the 60% cutoff lacks formal validation. Limitations include exclusion of women’s experiential perspectives, potential Hawthorne effects, absence of inter-observer reliability testing, and sampling constraints that reduce generalizability. The cross-sectional design limits causal inference, with wide confidence intervals reflecting modest sample size. Larger, longitudinal, mixed-methods studies are needed to validate findings and capture evolving service quality in conflict-affected settings.
CONCLUSION
This study highlights major deficiencies in antenatal care in Nyarambe, driven by supply shortages, limited diagnostics, and inadequate training. Future reforms must strengthen infrastructure, standardize protocols, and ensure continuous provider development. In fragile contexts, resilient supply chains, governance, and security strategies are essential to improve maternal and neonatal outcomes.
Acknowledgements
We are grateful to the School of Health Steering Committee, local authorities, providers, communities, and data teams, with special recognition to the field and analysis teams for their professionalism and commitment throughout.
Disclaimer
None.
Ethics statement
The study protocol was approved by the Ethics Committee of the School of Public Health, University of Kinshasa. Informed consent was obtained from all participants involved in the study.
Data availability
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Funding
This study received no external funding and was carried out using the researchers’ own funds.
Authorship contributions
-
Edebhati Bhaako Jean-Pascal – Corresponding author, responsible for study design, data analysis, and manuscript writing.
-
Bernard-Kennedy Nkongolo – Statistical analysis.
-
Donat-Soft Mukuna – Manuscript revision and critical reading.
-
Nelly Dikamba – Promoter, contributed to methodological supervision.
Disclosure of interest
The authors completed the ICMJE Disclosure of Interest Form and declare that they have no conflicts of interest related to this study