BACKGROUND
According to the World Health Organization (WHO), almost 800 women die daily due to pregnancy and childbirth-related factors, 69% of which come from the African region. Nigeria, the most populous African country, has one of the highest maternal mortality rates globally, standing at 1047 deaths per 100,000 live births as of 2020.1,2 In 2003, the World Health Organization recommended that a minimum of four ANC visits was adequate for pregnant women without complications.3 Although this number was increased to eight contacts in 2016,4 the 2021 MICS dataset used in this study considered the previously recommended four ANC visits as adequate likely due to the slow national progress in adapting to the 2016 recommendation. By 2018, only about 20% of pregnant women in Nigeria had utilized up to eight ANC or more visits with about 25% difference in utilization between urban and rural areas with significant inequalities across sociodemographic divides.5
Unequal access to maternal healthcare services contributes to disparities in health outcomes across Nigeria. Several studies have found that regions with lower ANC utilization rates often witness higher maternal and neonatal mortality rates and increased incidences of preventable complications during pregnancy and childbirth.6–9 Moreover, socioeconomic disparities play a significant role, with 86% of women from the wealthiest households having adequate ANC compared to only 18% from the poorest households.10 Maternal mortality and morbidity hinder economic development by reducing the productivity of women, exacerbating poverty levels, and perpetuating cycles of inequality. Addressing regional disparities in maternal healthcare access is thus not only a matter of social justice but also critical for achieving sustainable developmental goals pertaining to health and inequalities.11 Insights from the National Demographic and Health Survey in Nigeria, which was published in 2018 (over 6 years ago) suggest that socioeconomic status, cultural beliefs, and geographic location contribute to disparities in maternal healthcare access from a national level.12–19 Despite advancements in healthcare infrastructure and service delivery, the benefits have not been uniformly distributed, instead, inequities in health and healthcare have increased within regions over time.20,21
While previous literature have drawn attention to the disparities in maternal healthcare access from a national level, many of these studies did not assess for regional inequalities in ANC in the country and its associated factors.10,12,14 Hence, this study aims to fill in this research gap by providing updated insights from the recent Multiple Indicator Cluster Survey (MICS) 2021 data. Our study offers a comprehensive analysis of the current state of ANC utilization across different regions of Nigeria by leveraging this large dataset. Furthermore, this study contributes to the existing literature by emphasizing the importance of addressing regional disparities in maternal healthcare access for achieving sustainable development goals. Through evidence-based policy recommendations, our study will inform decision-makers and healthcare stakeholders on strategies to promote equitable access to ANC services and improve maternal and child health outcomes nationwide.
METHODS
Data
Data obtained from the Nigeria Multiple Indicator Cluster Survey (MICS), 2021 were utilized in this study. The MICS is a household survey programme developed by the UNICEF in the mid 90’s to assist countries in filling data gaps for monitoring the situation of children and women. The selection of countries and the choice of questions for the MICS is done in conjunction with the Demographic and Health Surveys (DHS).22 The MICS dataset is de-identified and publicly available on the UNICEF’s website.23 and as such no ethical approval or permission was sought before the commencement of the study. The MICS 2021 Nigeria survey is a nationally representative survey that was conducted to collect data on a wide range of social and demographic indicators which includes child health, maternal health, water, and sanitation, among others. The MICS 2021 survey employed a multistage, stratified cluster sampling design to ensure that the data is representative at the national and state levels. The survey covered all 36 states and the Federal Capital Territory of Nigeria, allowing for comprehensive and reliable insights into the country’s development progress and challenges. Information on women of reproductive age between the ages of 15 - 49 was used. However, data were grouped based on the six- geopolitical zones which formed the basis of comparison. After cleaning and sorting the data, a total of 6998 respondents’ data were used across all the regions.
Outcome measure
The outcome variable for this study was adequate ANC visits. Women with antenatal care visits of at least four had adequate ANC visits while less than 4 were inadequate. This study utilizes the four-visit antenatal care (ANC) model because data were drawn from the 2021 Multiple Indicator Cluster Survey (MICS), which was conducted before the WHO updated its recommendation to eight visits. At the time of data collection, the four-visit model was the globally recognized standard, making it the most appropriate framework for analyzing ANC coverage and maternal healthcare access. While the updated guideline reflects a shift toward enhanced maternal care, this study provides a valuable baseline for assessing ANC utilization prior to the transition.23 However, each region was independently evaluated.
Independent variables
Using the Andersen’s behavioural model,24 predisposing and enabling factors were identified from the respondents which were considered as covariates that may influence adequate ANC visit reflecting maternal and child healthcare service use. The predisposing factors include maternal age [15 – 24, 25 – 34, 35 – 44, 45 and above]; educational qualification (no education, primary, secondary, higher) and Wanting last child (Yes and No).While the enabling factors include wealth index (poorest, poor, middle, rich and richest), Health insurance (Yes and No), Area (Urban and Rural) Polygyny (Yes and No), Internet Usage (Yes and No), and Owning mobile phone (Yes and No).
Statistical analysis
Statistical Package for the Social Sciences (SPSS) version 27. First, descriptive analyses were done for all selected variables. Based on the regions, adequate and inadequate proportions were also evaluated. Finally, a multivariable binary logistic model was used to find out the adjusted effect of the independent variables on adequate ANC visits with a 0.05 level of significance.
RESULTS
Sociodemographic characteristics
Most of the respondents from the six geopolitical zones are from the age group 25-34 years. More than half of North East (NE) (845, 53.6%) and North West (NW) (1084, 59.7%) have no formal education while 75 to 80.9 percent of women in the Southern regions have at least a secondary education. Most of the respondents from the North Central (NC) (68.7%), North East (71.7%), North West (76.0%), South East (SE) (84.0%) and South-South (SS) (79.1%) are from rural settlements. The majority of the respondents do not utilize health insurance and have no internet usage (Table 1).
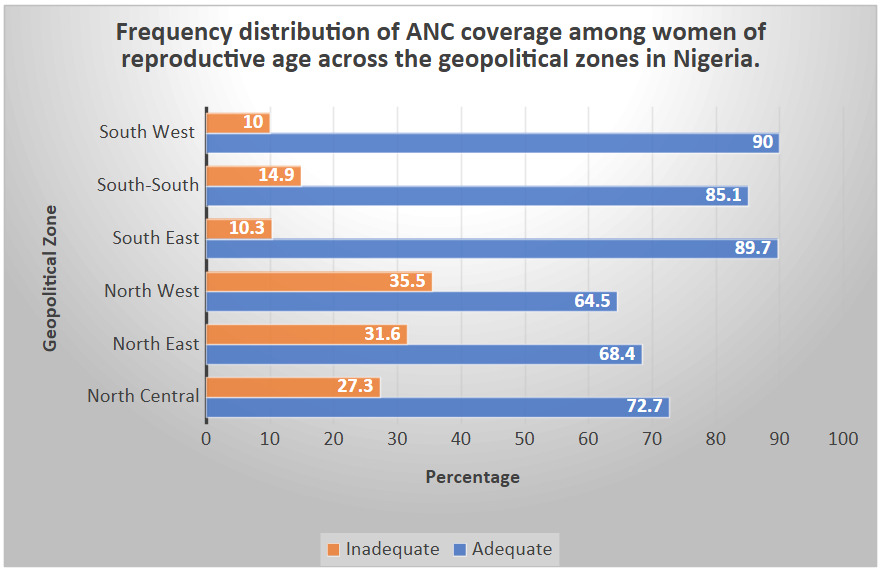
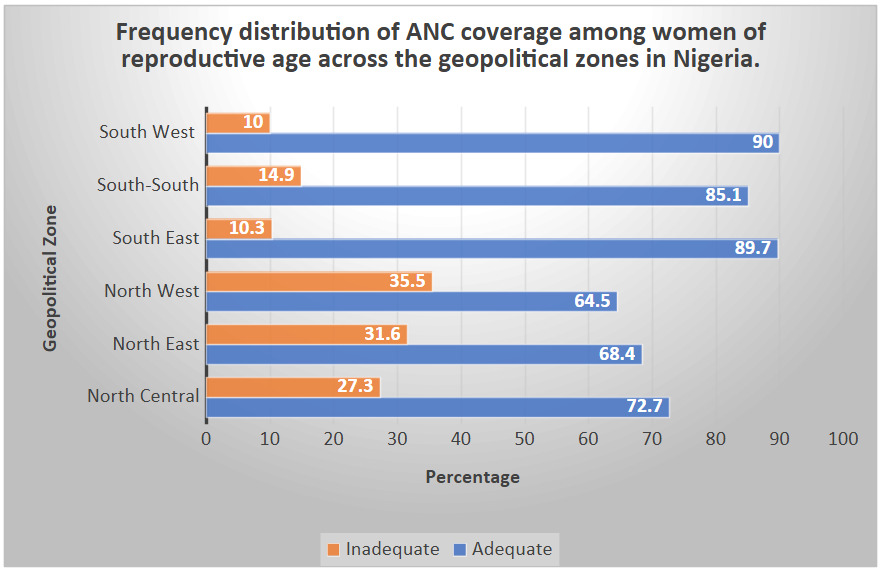
Regional inequalities in ANC Usage and Associated factors
Figure 1 summarizes the results from Table 2 depicting the adequacy of ANC usage across different regions of the country.
Respondents with primary, secondary, and higher/tertiary education from NE were 1.9 (CI: 1.3 – 2.7), 2.3 (CI: 1.7 – 3.1) and 2.1 (CI: 1.1 – 4.2) times more likely to adequately use ANC which was statistically significance. Those with with primary, secondary, and higher/tertiary education from NC were 1.2 (CI: 0.8 – 1.6), 2.1 (CI: 1.5 – 2.9) and 2.3 (CI: 1.2 – 4.1) times more likely to adequately use ANC and those from SS were 2.2 (CI: 0.7 – 7.4), 1.6 (CI: 0.5 – 5.1), and 6.7 (CI: 1.03 – 43.4) times respectively, more likely to adequately use ANC when compared with those with no formal education.
Also, respondents in the second, middle, fourth and richest wealth indexes in SW were 1.3 (0.573 - 3.027), 2.4 (0.972 - 6.075), 3.2 (1.207 - 8.667) and 5.4 (1.644 - 17.559) times respectively more likely to adequately utilize ANC than those in the poorest wealth index while their counterparts in the NW with the same respective wealth indexes were 1.0 (0.791 - 1.292), 1.6 (1.197 - 2.226), 2.7 (1.783 - 4.235) and 3.3 (1.712 - 6.539) times more likely to adequately use ANC.
The logistics regression result shows that respondents from SW with 6 or more children are 70% less likely to utilize ANC compared to those with 1-3 children (OR= 0.3, CI= 0.113 - 1.037). Respondents from NE, NW, SE, and SS who are not in polygynous marriages are 40%, 10%, 20%, and 30% respectively, more likely to adequately utilize ANC than those who are in polygynous marriages. Women who do not use the internet from NW, SE, SS, and SW are 30%, 10%, 40%, and 50% respectively, less likely to adequately use ANC than those who utilize the internet. Across all regions, those who do not have a mobile phone are 20% to 40% less likely to adequately utilize ANC than those with a mobile phone. Women from the NC, NE, SE, SS, and SW who did not want their last child are 30%, 20%, 10%, 40%, and 40% respectively, less likely to adequately utilize ANC than those who wanted their last child. Women from the NC, NE, SS, and SW who do not utilize health insurance are 70%, 60%, 40%, and 10% respectively less likely to adequately utilize ANC than those with health insurance (Table 3).
DISCUSSION
This study assessed the inequalities in ANC use in Nigeria, focusing on the regional differences, using the most recent nationally representative data from MICS 2021. Our results provided a comprehensive overview of the sociodemographic characteristics of respondents across Nigeria’s six geopolitical zones. Notably, it highlights distinct disparities between the Northern and Southern regions, particularly concerning education levels, reproductive age distribution, wealth index, and access to healthcare services. These findings are consistent with previous research that has established the disparities between the Northern and Southern regions of the country in terms of developmental indices.23,25
Owning a mobile phone is associated with adequate utilization of ANC compared with not having a mobile phone. While previous studies have established the positive relationship between mass media exposure and ANC care usage, the 21st-century advent of mobile phones and the internet in the country has changed the tides of communication.19 A lot of health information and awareness interventions are becoming more digitalized including those focused on maternal health. This disparity in access to information is likely to have led to a disparity in behavioral change affecting health services uptake including ANC. While a lot of health interventions are being digitalized, targeted interventions need to be designed and reinforced to reach people in less technologically developed areas, especially in the North East and North West, where more than half of the respondents do not have access to mobile phones. The results also suggest that improving internet access nationwide is likely to increase the adequate usage of ANC.
A clear North-South disparity existing in antenatal care (ANC) utilization across Nigeria, with better usage observed in the southern region has been attributed to differences in culture, education, and religion.13,17,26 Educational attainment plays a crucial role in maternal healthcare service utilization, as studies have shown a positive correlation between higher education levels and ANC usage.13,19,26 Women with at least a primary school education, except in the South-East (SE) and South-West (SW), are more likely to adequately utilize ANC. Likewise, younger maternal age (15–24 years) is associated with a lower probability of attending at least four ANC visits, a trend closely linked to educational attainment. Women with higher education tend to marry later, achieve financial independence, and have greater awareness of ANC services, all of which contribute to increased utilization.13,26 Cultural norms in the Northern region further exacerbate gender inequality, as studies have shown a negative correlation between residency in the North and gender equity.27 This is reflected in higher rates of early marriage and lower rates of female education in the region.28 To improve ANC utilization, expanding access to education, particularly in the North, is essential. Evidence also supports the involvement of religious and community leaders in implementing health interventions and promoting girl-child education, both of which could contribute to increasing adequate ANC attendance to at least four visits.29,30
Women who did not want their last child and women with more than four children showed higher odds of inadequate ANC utilization. A systematic review in Africa supports this finding as it was discovered that pregnancy planning and wantedness improve the adequate utilization of ANC and conversely, women with unplanned/unwanted pregnancies were less likely to adequately utilize ANC.16 Women with higher parity may consider themselves experts and hence delay attending ANC in their subsequent pregnancies. Other suggested reasons to explain the association of high parity with inadequate ANC usage include the burden of caring for other children leaving less time available for ANC, and negative experience from previous ANC.26
Women from the lower wealth index are less likely to adequately utilize ANC. Less than 8% of Nigerians are covered by the national health insurance scheme, and more than 70% of Nigerians do out-of-pocket services.31–33 The high level of poverty in the country34 therefore makes it difficult for an early uptake of ANC services, despite subsidization of the fees.32,35 This finding reveals the need to improve the affordability of healthcare in the country, including maternal healthcare and increasing the coverage of health insurance. Women not in polygynous marriages were found to utilize ANC services up to at least 4 times during pregnancy compared to women in polygynous marriages. While studies have shown that being married is significantly associated with ANC usage,36 there have been contrasting reports on whether the kind of marital union affects ANC usage36,37 Nigeria has made efforts to improve ANC utilization with the implementation of programs such as the Maternal, Newborn, and Child Health (MNCH) Week which is a biannual event that provides free antenatal care, immunizations, and other essential health services to pregnant women and children and the Conditional Cash Transfer programs that provide cash incentives to pregnant women who attend the recommended number of antenatal visits and deliver at a health facility, however, there has been slow progress across some regions.36 [40, 41]
This study has implications for the planning and implementation of healthcare, educational programs and technological interventions in the country. The association between mobile phone ownership and adequate ANC utilization underscores the growing role of digital health interventions in improving maternal healthcare in Nigeria. However, the digital divide, particularly in the North-East and North-West where mobile phone access is low, poses a challenge to equitable healthcare access. As health interventions become increasingly digitalized, strategies must ensure inclusivity by integrating mobile-based health education, SMS reminders, and telehealth services while also leveraging alternative communication channels like community radio and local health workers. Expanding internet access and improving mobile phone affordability will further enhance ANC uptake, reducing maternal health disparities nationwide. Educational disparities between the North and the South need to be addressed to see an increase in the utilization of maternal healthcare services through targeted educational programs and policies implemented in the Northern regions of the country. Gender equality needs to be taken into account, encouraging the education and economic empowerment of the girl-child. Sustained and improved effort is necessary to improve the coverage of the NHIS and other insurance schemes which is necessary to make affordability of maternal healthcare services across the regions equitable.
Strengths and Limitations
The major strength of this study lies in the cost-effectiveness and large sample size of women in the reproductive age group by utilizing the most recent data on ANC utilization using the MICS 2021 data. Furthermore, to our knowledge, this study is the first to examine regional inequalities in ANC in Nigeria and its associated factors using the MICS 2021 data. This provides nationally and regionally representative data allowing for better comparison across regions. Hence, our study is well suited to guide and inform regional and national policies especially on ANC, reproductive health and public health. However, a limitation of this study is the MICS (the secondary data) used may be subject to recall bias. Another limitation of the data is the reporting of the data based on the old minimum of four ANC visits recommended by the WHO instead of the more recent eight minimum encounters.
CONCLUSIONS
Our study provides evidence of persisting regional disparities in antenatal care utilization in Nigeria, signaling the importance of evidence-based interventions tailored to address the unique challenges faced by each region to ensure equitable access to maternal healthcare services. Addressing these disparities requires a holistic approach that takes into account the socioeconomic, cultural, and infrastructural challenges specific to each region. Targeted interventions aimed at improving access to mobile phones, internet and mass media are becoming increasingly important just as education, economic empowerment and healthcare infrastructure are, for achieving equitable ANC utilization and ultimately improving maternal and child health outcomes nationwide.
Acknowledgement
Nil
Funding
No funding was received for this study
Authorship Contributions
IO and RO conceptualized the study. IO and PA were involved in the data analysis. PA and RO were involved in the literature review and wrote the first draft of the manuscript. PA, RO, and MA were involved in writing the second and third draft of the manuscript. IO, PA, RO, MA, EO and IA were involved in the review and editing of the manuscript. IO, PA, RO, MA, EO, and IA were involved in writing the final manuscript draft. All authors contributed to the original draft of the manuscript.
Disclosure of Interest
The authors completed the ICMJE Disclosure of Interest Form (available upon request from the corresponding author) and disclose no relevant interest/declare the following activities and relationships
Correspondence to
Ruth Oladele
Department of Center for Excellence in Modelling Population health and Environment Risks (CEMPHER), Slum and Rural Health Initiative
Ibadan
Nigeria
ruth.oladele@srhin.org