Family planning (FP) is recognized as a cornerstone of public health, reducing maternal and infant morbidity and mortality while enabling families to achieve their reproductive goals.1,2 It empowers couples to determine the number of children they desire, the timing of births, and appropriate spacing, thereby fostering optimal child growth and family well-being.3,4 Despite these benefits, FP remains a complex issue at the intersection of health, social, cultural, and religious concerns. While widely acknowledged as a solution to unwanted pregnancies and maternal deaths, it is often perceived as a challenge to traditional norms and community beliefs.5,6
Globally, the World Health Organization (WHO) estimates that a woman dies every two minutes from pregnancy or childbirth complications, amounting to more than 260,000 deaths annually, with 70% occurring in sub-Saharan Africa.7 Each year, approximately 73 million abortions are performed worldwide.8 In 2019, modern contraceptive use prevented 218 million unintended pregnancies, 138 million abortions, and 118,000 maternal deaths.3 Of the 1.9 billion women of reproductive age (15–49 years), 842 million use modern contraception, yet 270 million still have unmet needs.9 In 2022, global modern contraceptive prevalence was 77.5%, compared to only 58% in sub-Saharan Africa.2
In the Democratic Republic of Congo (DRC), Demographic and Health Surveys (DHS 2013–2014; DHS 2023–2024) show a modest increase in modern contraceptive prevalence, from 7.8% to 11% among married or unionized women.10,11 Common methods include male condoms (9%), emergency contraception (4%), pills (3%), and implants (3%), while the rhythm method remains frequent (4%).11 Despite national commitments through the “Desired Births” initiative (1972), its repositioning in 2004, and the Addis Ababa conference in 2013,12 challenges persist: Congolese women average 5.5 children,11 24% report unmet FP needs,13 and maternal mortality remains high at 841 deaths per 100,000 live births.10,11 In Kinshasa, modern contraceptive prevalence is 9.12%, but only 4.44% in the N’djili health zone, far below the national target of 20%.13,14
Despite systematic reviews and meta-analyses highlighting the effectiveness of FP interventions in reducing maternal risks, gaps remain in understanding the local determinants of contraceptive uptake, particularly in urban health zones with low prevalence. This study therefore aims to identify factors influencing modern contraceptive use among women aged 18–49 in N’djili, to strengthen FP strategies and contribute to reducing maternal morbidity and mortality in the DRC
II. METHODS
2.1. STUDY FRAMEWORK
The study was conducted in the N’djili Health Zone (HZ), located southeast of Kinshasa. Covering 11.2 km², it serves a population of 425,843 inhabitants. The zone is organized into 14 health areas (HAs) and includes a General Referral Hospital alongside 205 healthcare facilities. Its mission is to provide primary healthcare to a population characterized by high density (36,915 inhabitants/km²).
2.2. DESIGN AND PERIOD OF STUDY
We carried out a cross-sectional analytical study. Data collection occurred from May 1 to June 1, 2025.
2.3. SAMPLING
2.3.1. Study Population
The study population consisted of women of childbearing age (18–49 years) residing in N’djili.
-
Inclusion criteria: Women aged 18–49, residing in the zone during the study, and consenting to participate.
-
Exclusion criteria: Pregnant women (MCM use not applicable), women with cognitive impairments, or serious health conditions preventing participation.
2.3.2. Sample Size
The sample size was calculated using Fisher’s formula:
-
p = 9.12% (prevalence of modern contraceptive use in Kinshasa, DHIS2 2024)
-
Z = 1.96 (95% confidence interval)
-
d = 0.05 (margin of error)
The minimum sample size was 128 participants. This was adjusted by a design effect of 2.5 to account for intra-cluster correlation across five health areas, then weighted demographically to reflect population densities. A 10% margin for non-response was added, yielding a final sample of 394 women. This ensured statistical power and representativeness within Kinshasa’s complex urban context.
2.3.3. Sampling Technique
A three-stage probability sampling method was applied:
-
Clusters: From 14 health areas, 5 were randomly selected, with proportional allocation to population size.
-
Avenues: Within each selected HA, 3 avenues were randomly chosen, weighted by demographic density.
-
Households/Respondents: Households were systematically sampled at fixed intervals. In each, one eligible woman was interviewed; if multiple met criteria, one was randomly selected.
This design yielded 394 women, ensuring representativeness and statistical rigor.
2.4. STUDY VARIABLES
2.4.1. Dependent Variable
- Use of a Modern Contraceptive Method (MCM): Dichotomous (Yes/No).
2.4.2. Independent Variables
Grouped into five dimensions:
-
Sociodemographic characteristics: Age, education level (none/primary, secondary, tertiary), religion (Christian/Other), occupation (formal/informal/unemployed), parity (number of children).
-
Knowledge of MCMs: Sources of information, methods known, perceived advantages/side effects. Knowledge was “good” if ≥5 methods cited, “poor” if <5.
-
Practices: Types of MCM used, motivations (spacing/limiting), barriers (spousal opposition, religious reasons). Practices measured as current use (Yes/No) and history (ever/never).
-
Perceptions: Opinions on contraception and reproductive health. Perception was “good” if methods were seen as advantageous, “poor” if linked to side effects.
-
Household socioeconomic status: Measured via an asset index. Principal Component Analysis (PCA) classified households into tertiles: poor, middle, rich.
2.5. DATA COLLECTION
Data were collected through face-to-face interviews using a pre-tested structured questionnaire. To enhance accuracy, the tool was digitized and administered via KoboCollect, enabling real-time entry and monitoring. Four teams of trained interviewers conducted household visits, following standardized procedures to minimize bias. Supervisors regularly checked entries for completeness and consistency, ensuring data quality.
2.6. DATA PROCESSING AND ANALYSIS
Data exported from KoboCollect to Excel were analyzed using SPSS version 27.
-
Descriptive analysis: Categorical variables were presented as frequencies/percentages; numerical variables as mean ± SD (normal distribution) or median with interquartile range (skewed).
-
Missing data: Assessed systematically; incomplete responses excluded from specific analyses. Sensitivity checks ensured no bias.
-
Inferential analysis: Associations between independent variables and MCM use were tested using Pearson’s chi-squared or Fisher’s exact test when appropriate. Variables with p < 0.20 in bivariate analysis were retained for regression; those with p < 0.05 were considered significant.
-
Multivariate analysis: Logistic regression identified determinants of MCM use, adjusting for confounders. Odds ratios (ORs) with 95% confidence intervals (CI) were calculated. Multicollinearity was tested using Variance Inflation Factors (VIF); variables with VIF > 10 were excluded or adjusted. Candidate variables were selected based on literature review and theoretical relevance.
2.7. ETHICAL CONSIDERATIONS
The study was approved by the Ethics Committee of the School of Public Health (No. ESP/CE/90/2025). Written or verbal informed consent was obtained before interviews. Anonymity and confidentiality were strictly guaranteed. Participation was voluntary, with the option to withdraw at any time without penalty
III. RESULTS
3.1. SOCIODEMOGRAPHIC AND SOCIOECONOMIC CHARACTERISTICS OF WOMEN AGED 18-49 YEARS
Among the 394 women aged 18 to 49, the majority reside in Ward 5 (32.5%) and are primarily in the 25-29 age bracket (27.7%). The most common level of education is completed secondary school (44.2%), while nearly half are married (48.5%). The most represented occupational category is homemaker (30.2%). The dominant religion is the Pentecostal Church (64.7%). Regarding family composition, most have one child (25.4%) and live in households of fewer than six people (51.3%). Finally, almost all spend more than 3,500 FC per day on food (98%) and the majority belong to the middle wealth Tertile (41.4%).
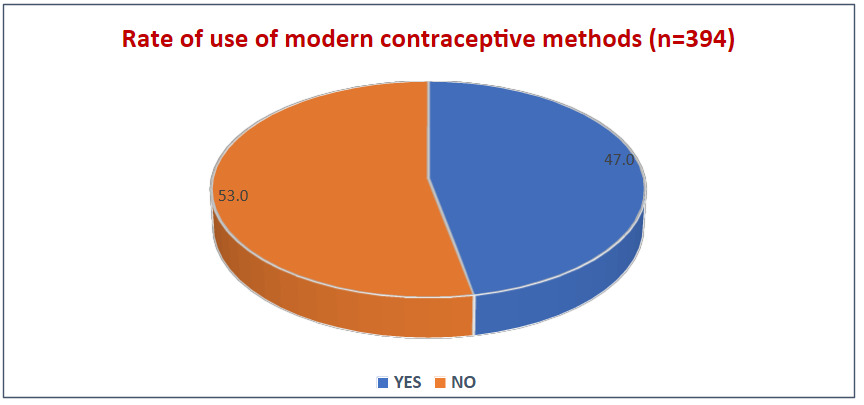
3.2. RATE OF USE OF MODERN CONTRACEPTIVE METHODS (MCM)
_among_women_aged_18-49_years_in_the_ndji.png)
3.3. WOMEN’S KNOWLEDGE OF MCMS
Table II shows high awareness, with 97.7% of women having heard of modern contraceptive methods, mainly via health facilities (55.1%) and neighbors (45.7%). While 91.4% know different methods, knowledge favors hormonal options—pills (61.4%), implants (54.6%), injectables (49%)—over condoms (45.2%). Long-acting methods like IUDs (8.9%) and vasectomies (0.5%) remain rare, underscoring the need for broader communication to ensure informed choice.
3.4. FACTORS ASSOCIATED WITH THE USE OF MCM
The Significant associations were observed for health area, occupation, number of children, household wealth, prior awareness, and knowledge of modern contraceptive methods.
Multivariate analysis shows that only economic status and knowledge independently determine MCM use. Women in poor (aOR=0.34; p=0.002) and middle (aOR=0.52; p=0.037) tertiles, and those lacking knowledge (aOR=0.08; p=0.001), are significantly less likely to adopt contraception, highlighting financial insecurity and limited information as key barriers in N’djili.
IV. DISCUSSION
4.1. KEY RESULTS OF THE STUDY
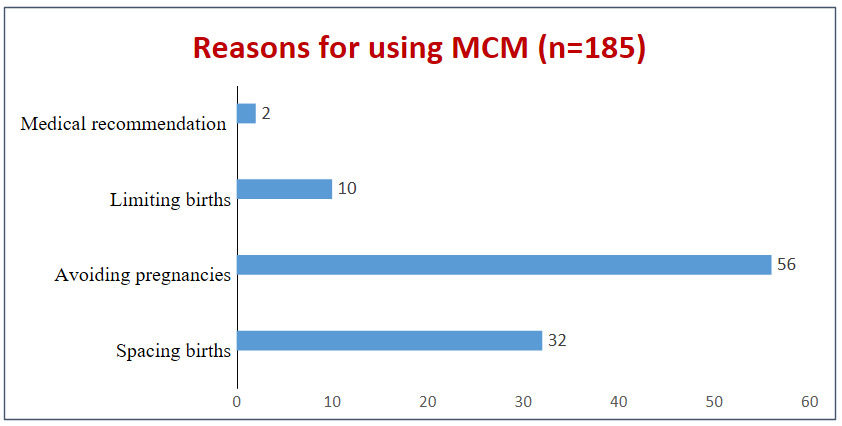
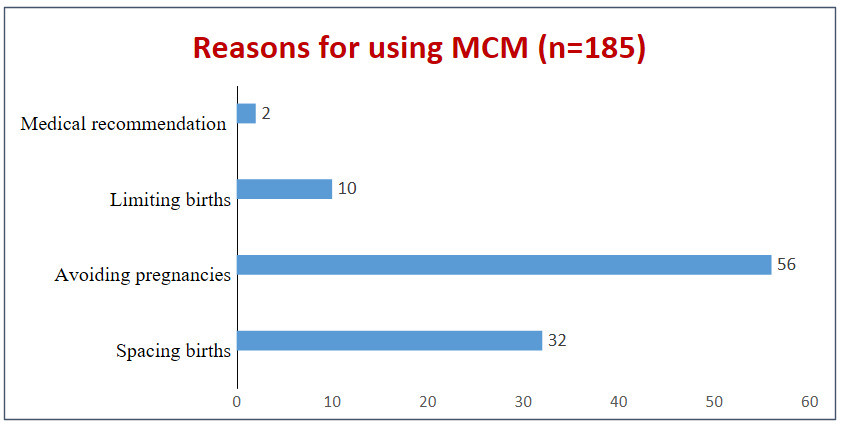
ThisThis study in the Ndjili health zone found that 47% of women aged 18–49 use modern contraceptive methods, mainly to prevent pregnancy (56%) or space births (32%). Awareness is high (97.7%), with knowledge concentrated on pills (61.4%), implants (54.6%), and injectables (49%). After adjustment, only economic status and technical knowledge remained independent determinants: poor (aOR=0.34) and middle-class (aOR=0.52) women, and those lacking knowledge (aOR=0.08), were significantly less likely to use MCMs. Financial insecurity and limited information emerged as the main barriers to modern contraception
4.2. RATES AND REASONS FOR USE OF MODERN CONTRACEPTIVE METHODS
The The prevalence of modern contraceptive method (MCM) use in Ndjili (47%) is markedly higher than the national averages reported by the 2023 DHS (21% of demand met by modern methods) and the 2014 DHS-DRC (19%) [25–27]. This indicates faster progress compared to the national trend, which remains below 30%. In our study, household-based data revealed a prevalence of 47%, while DIHS2 reported only 4.44%. This discrepancy reflects differences in data sources: DIHS2 compiles hospital-based statistics, excluding women who access MCMs through private providers or pharmacies. Household surveys therefore provide a more comprehensive estimate of actual use.
Intra-urban disparities remain evident. Mputu et al. observed a 55% prevalence in another Kinshasa area, suggesting that socio-economic vulnerability and access to practical information strongly influence adoption.15 Comparatively, Ndjili performs better than many urban areas in West Africa, surpassing the 38% reported in Burkina Faso.16
Regarding reasons for use, most women in Ndjili adopt MCMs to avoid pregnancy (56%), followed by birth spacing (32%). This aligns with national data: the 2023 DHS reported unmet needs of 22% for spacing and 10% for limiting births [25]. The 2018 MICS confirmed that birth control is a strong driver of adoption in precarious urban contexts, while Hamadou et al. in Niger highlighted how economic constraints reinforce the desire to limit family size.17 These findings underscore the importance of leveraging high adoption rates to further promote birth spacing, emphasizing its health benefits for mothers and children.7,18
4.3. WOMEN’S KNOWLEDGE OF MCMS
Findings In Ndjili, awareness of modern contraceptive methods (MCMs) is nearly universal (97.7%), comparable to the 2023 DHS (91.2%).14 However, knowledge is selective: pills (61.4%), implants (54.6%), and injectables (49%) dominate, while IUDs (8.9%) and vasectomy (0.5%) remain marginal. The 2018 MICS highlighted similar gaps, with less educated women less exposed to long-duration methods (LDMA).18 Studies in Nigeria and Ethiopia confirm that unequal access to knowledge limits informed choice [Kasso; Zeleke]. LDMA, despite lower discontinuation rates (30% vs. 64–68% for pills/injectables),14 is poorly promoted. Only 30% of users received comprehensive counseling, dropping to 13% among pill users. Information mainly comes from health facilities (55.1%) and social networks (45.7%), consistent with findings in Tanzania.19 Strengthening provider communication and expanding counseling on LDMA is crucial to transform general awareness into informed, sustainable contraceptive use.
4.4. FACTORS ASSOCIATED WITH THE USE OF MCMS
In Ndjili, awareness of modern contraceptive methods (MCMs) is nearly universal (97.7%), comparable to the 2023 DHS (91.2%) [DHS 2023]. Yet knowledge remains selective, with pills (61.4%), implants (54.6%), and injectables (49%) dominating, while IUDs (8.9%) and vasectomy (0.5%) are marginal. The 2018 MICS highlighted similar gaps, showing that less educated women are less exposed to long-duration methods (LDMA) [MICS 2018]. Studies in Nigeria and Ethiopia confirm that unequal access to knowledge limits informed choice [Kasso; Zeleke]. Despite LDMA’s lower discontinuation rates (30% vs. 64–68% for pills/injectables) [DHS 2023], promotion remains weak.
Counseling is also insufficient: only 30% of users reported receiving comprehensive information, dropping to 13% among pill users. In Ndjili, health facilities (55.1%) and social networks (45.7%) are the main sources of information, consistent with findings in Tanzania [Mkwananzi]. These channels represent strategic opportunities to strengthen provider communication and expand counseling on all available options, particularly LDMA. Moving from general awareness to informed, sustainable contraceptive use requires addressing these gaps in knowledge and counseling.
4.5. STRENGTHS AND LIMITATIONS OF THE STUDY
This study’s strengths include a robust sample size (394 women) and multivariate analysis of diverse sociodemographic and economic factors, enhancing reliability. Statistical methods such as chi-squared tests and logistic regression strengthened validity. However, the cross-sectional design limits causal inference, self-reported data risk recall and desirability bias, and restriction to one health zone reduces generalizability. Cultural norms and partner influence were not explored.
CONCLUSION
This study shows that fewer than half of women in Ndjili use modern contraceptive methods, despite widespread awareness. Use is mainly motivated by pregnancy prevention and birth spacing, but knowledge remains uneven, with hormonal methods dominating over long-acting options. Multivariate analysis identifies socioeconomic status and technical knowledge as key determinants. Persistent economic and informational barriers, alongside unexamined cultural and partner influences, highlight the need to strengthen counseling, expand information dissemination, and reduce inequalities to improve contraceptive adoption.
Acknowledgements
We are grateful to the women of the N’djili Health Zone who participated in this study, as well as the local health authorities and community leaders who facilitated data collection.
Disclaimer
The views expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the University of Kinshasa or the Ministry of Health of the Democratic Republic of Congo.
Ethics Statement
This study received ethical approval from the Ethics Committee of the School of Public Health, University of Kinshasa (Approval No. [insert number]). Written informed consent was obtained from all participants prior to their inclusion in the study.
Data Availability
The datasets generated and analyzed during the current study are not publicly available due to confidentiality agreements but are available from the corresponding author on reasonable request.
Funding
This research received no external funding. The article publication charge (APC) was not funded by any external source.
Authorship Contributions
-
Huguette Abasafiki Binti: Conceptualization, methodology, data collection, analysis, and drafting of the manuscript.
-
Hakim Kadima Musasa: Critical revision of the manuscript.
-
Rodriguez Mboma: Critical revision of the manuscript.
-
Prince Kimpanga Diangs: Supervision, critical revision of the manuscript, and final approval of the version to be published.
Disclosure of Interest
The authors completed the ICMJE Disclosure of Interest Form. No conflicts of interest were reported