BACKGROUND
Abdominal obesity has become a critical global public health concern, affecting not only overweight or obese individuals but also those with a normal Body Mass Index (BMI).1 This paradox—normal BMI yet excessive visceral fat—poses a growing challenge, with an estimated 650 million obese adults worldwide in 2022, many presenting central fat accumulation despite normal BMI.2
In Africa, the burden of abdominal obesity is rising sharply, driven by urbanization, dietary transitions, and sedentary lifestyles. In sub-Saharan Africa, about 30% of urban adults are affected.3 In the Democratic Republic of Congo (DRC), although national data remain limited, regional studies consistently highlight increasing prevalence, particularly among women and urban populations.4 This underscores the urgent need for localized evidence to guide interventions.
Determinants of abdominal obesity are multifactorial, encompassing poor diet and physical inactivity,5 genetic and hormonal predispositions,6,7 and psychosocial stressors such as sleep disturbances and socioeconomic constraints.8,9 These factors interact to promote visceral fat accumulation, heightening risks of cardiometabolic complications.
Abdominal obesity is strongly linked to cardiovascular disease, type 2 diabetes, hypertension, and dyslipidemia,10 while also contributing to psychosocial distress11 and escalating health care costs.12 Recommended strategies include promoting physical activity,13 encouraging balanced diets,14 and ensuring regular medical monitoring,15 alongside broader public health policies to reshape dietary and lifestyle behaviors.16
A major challenge remains the lack of precise epidemiological data, particularly in urban contexts such as Gombe Matadi. Without such evidence, health policies risk being poorly tailored to local realities.17 This study therefore aims to identify factors associated with abdominal obesity among adults with normal BMI in Gombe Matadi, providing clinicians and policymakers with actionable insights for prevention and early detection.
II. METHODS
TYPE OF STUDY
This research was a secondary analysis of data from a cross-sectional survey conducted in 2019 in Gombe Matadi.
STUDY FRAMEWORK
The study was carried out in the Gombe Matadi health zone, located in Kongo Central province, Democratic Republic of Congo.
STUDY POPULATION
The population included Congolese adults aged 19 years and older, residing in the Gombe Matadi health zone, regardless of gender. Only participants with a normal BMI (18.5–24.9 kg/m²) and complete anthropometric data were retained. Restricting to normal-BMI adults allowed exploration of the paradox of abdominal obesity in individuals not classified as overweight, thereby identifying a context-specific risk profile relevant for targeted screening and counselling.
SAMPLING
A) SAMPLE SIZE The sample size was calculated using the formula:
n=Z2pqgd2×11−f
Where:
-
f=0.10 (non-response fraction)
-
Z=1.96 (95% confidence coefficient)
-
p=0.05 (frequency found in Kisantu, Muyer T., 2007)
-
q=0.95
-
d=0.02 (precision)
-
g=2 (cluster effect correction, Couloumbier et al., n.d.; United Nations, 2010)
This yielded n=912. After adjusting for non-response, the sample was 1013. To comply with STEPwise methodology requiring ≥1600 participants (STEPwise, 2008), 1700 individuals were selected. For this secondary analysis, 1039 subjects with normal BMI were retained. Post-hoc power analysis confirmed >80% power to detect moderate associations.
B) SAMPLING TECHNIQUE The main survey used a four-stage cluster probability design:
-
Five health areas (Gombe-Matadi, Yanda, Mbanza Nzumbi, Ntimamfi) were purposively selected due to diabetes program involvement, introducing potential selection bias.
-
One neighborhood was randomly chosen per area, followed by proportional sampling of plots using systematic intervals.
-
Households were randomly selected within plots.
-
One eligible subject was randomly chosen per household.
Non-response was managed by replacing households after three failed contact attempts. For this secondary analysis, only normal-BMI individuals were retained, introducing convenience sampling at this stage and limiting representativeness.
DATA COLLECTION
Authorization was obtained from RIPSEC project managers, and the ESPK Ethics Committee approved the protocol. Data were extracted on:
-
Anthropometry: weight, height, waist circumference
-
Sociodemographics: age, gender, marital status, education, occupation
-
Health behaviors: alcohol, smoking, sedentary lifestyle, diet
Abdominal obesity was defined using WHO sex-specific waist circumference cut-offs (≥94 cm men, ≥80 cm women). Measurements were taken with participants standing upright, feet together, arms relaxed, breathing normally. A non-elastic tape was placed midway between the lowest rib and iliac crest. Health behaviors referred to the past 30 days (smoking, alcohol) and past 7 days (sedentary time, diet).
DATA PROCESSING AND ANALYSIS
Descriptive statistics summarized categorical variables as frequencies/percentages and continuous variables as means ± SD or medians with interquartile ranges. Multivariate logistic regression identified factors associated with abdominal obesity. Variables entered the model if theoretically relevant or significant at p < 0.20 in bivariate analysis. Multicollinearity was checked (VIF < 2). Missing data were handled by complete-case analysis. Model fit was assessed with the Hosmer–Lemeshow test, and diagnostics included residual analysis. Adjusted odds ratios (AORs) with 95% confidence intervals (CIs) were reported. Survey design and sampling weights were applied.
ETHICAL CONSIDERATIONS
The ESPK Ethics Committee approved this secondary study (No.ESP/CE/60/2025. Data were anonymized, with participant names excluded from the database. Confidentiality was strictly maintained, and participation was voluntary. The results of this study will not be used for commercial or political purposes.
RESULTS
SOCIODEMOGRAPHIC CHARACTERISTICS
Among the 1,039 adults with normal BMI, women represented 50.8%, and most were aged ≥40 years (69.9%). Two-thirds were married (66%), over half identified as Kimbanguists (53.8%), and nearly seven in ten reported farming as their main occupation (69.4%) (Table I). These distributions reflect the demographic profile of the study area rather than specific risk factors.
MEDICAL HISTORY AND BEHAVIORS
About one-quarter reported smoking (24.4%), while 28.2% consumed alcohol. Diabetes was present in 15.1%, hypertension in 9.9%, and 15.1% reported a sedentary lifestyle (Table II). These exposures provide contextual background for regression analysis.
PREVALENCE OF ABDOMINAL OBESITY
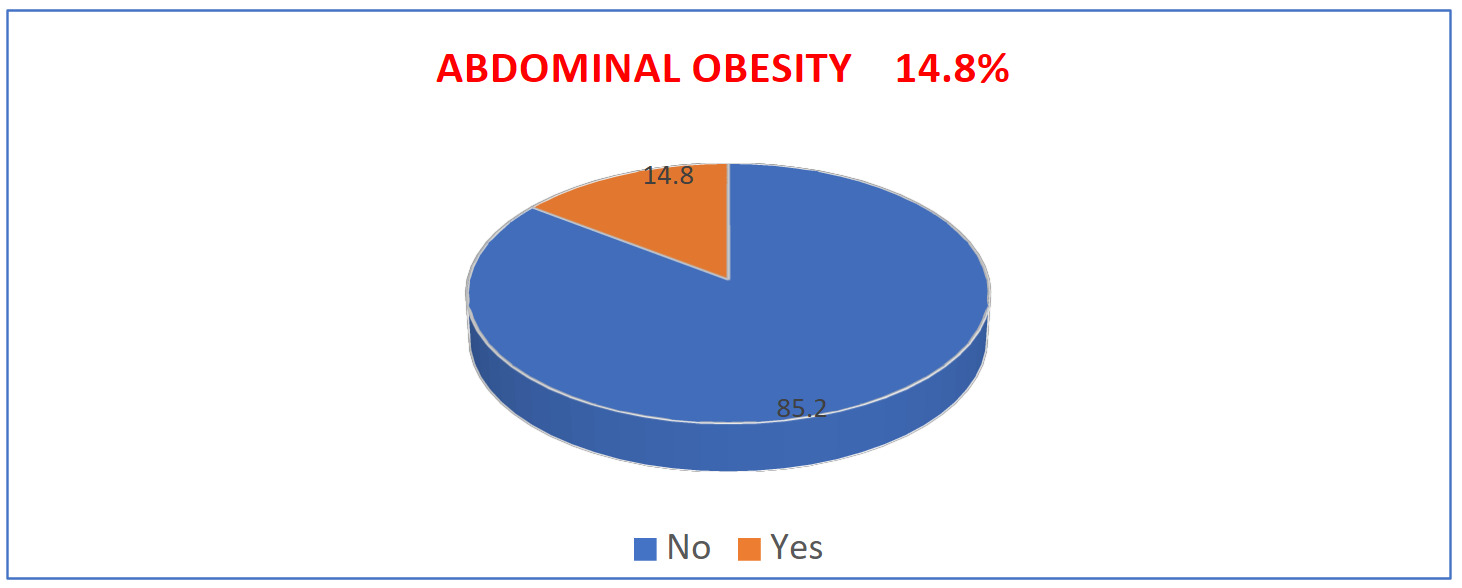
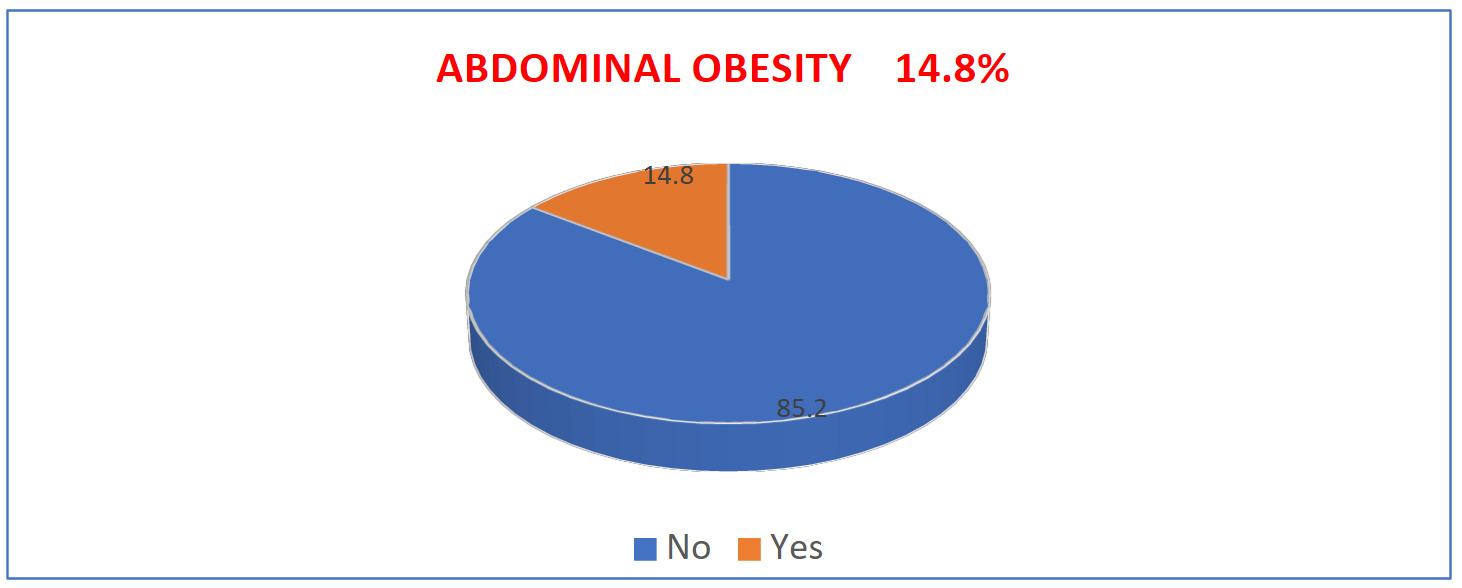
Overall, 154 individuals (14.8%) met criteria for abdominal obesity based on sex-specific waist circumference cut-offs (Figure 1), confirming that a notable proportion of normal-BMI adults carry excess visceral fat.
DIETARY HABITS
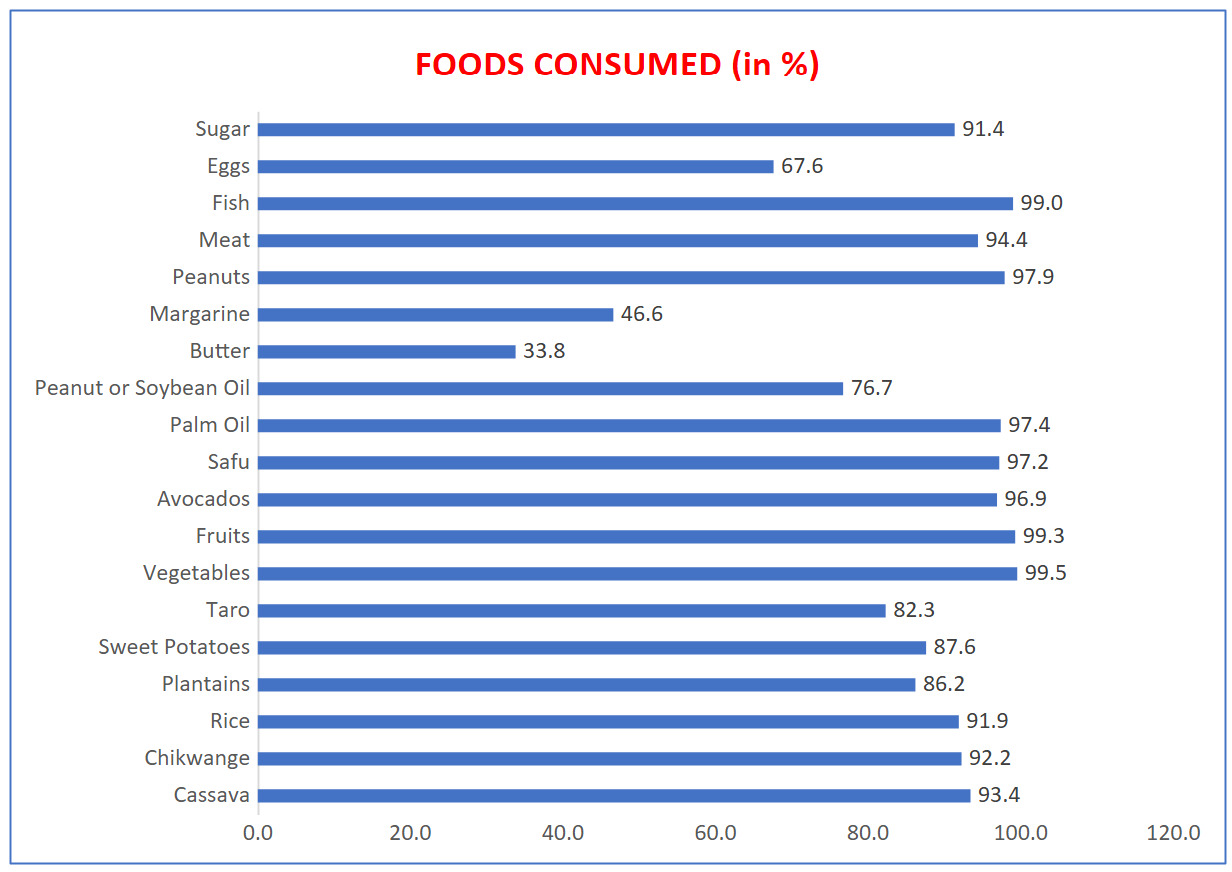
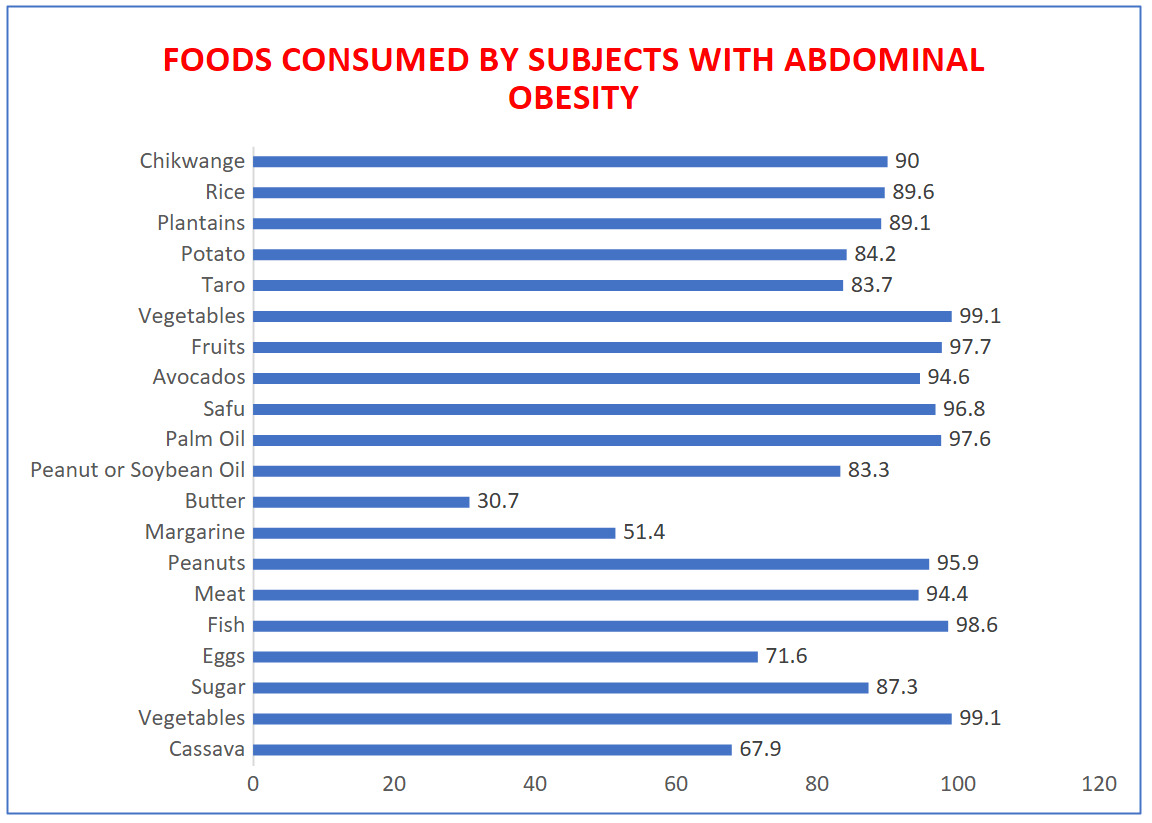
Dietary patterns were broadly similar across groups, with high consumption of cassava, chikwangue, rice, and plantain (>85%), and near-universal intake of vegetables, fruits, fish, and meat (>95%). Differences between groups were minimal, and the absence of portion size or nutrient composition data limits interpretation (Figures 2–3).
FACTORS ASSOCIATED WITH ABDOMINAL OBESITY
Bivariate analysis identified sex, age, education, smoking, sedentary lifestyle, and hypertension as associated factors (Table III). After adjustment, some associations shifted markedly. Men showed a crude OR of 0.025 (95% CI: 0.010–0.062), but adjusted OR rose to 5.376 (95% CI: 2.879–16.808), likely reflecting confounding or collinearity. Age <40 years remained a strong predictor (ORa = 4.945; 95% CI: 2.829–8.645). Secondary and higher education were protective (ORa = 0.531 and 0.554). Smoking (ORa = 1.982), sedentary lifestyle (ORa = 0.534), and hypertension (ORa = 2.034) were significant risk factors, while occupation and alcohol showed inconsistent associations.
TABLES AND FIGURES
_among_adults_with_normal_bmi_in_.png)
_in_adults_with_abdominal_obesity.png)
IV. DISCUSSION
OVERVIEW
In the Gombe Matadi health zone, abdominal obesity is a notable public health issue, even among adults with a normal body mass index (BMI). Of 1,039 participants, 50.8% were women and 69.9% were aged ≥40 years. The analysis revealed that 14.8% of adults with normal BMI had abdominal obesity (Figure 1), underscoring the limitation of BMI as a sole indicator of health status and highlighting the need to incorporate waist circumference into routine screening.18 Several factors were associated with abdominal obesity, including age, sedentary lifestyle, smoking, hypertension, and education level. These associations should be interpreted as correlations rather than causal pathways, given the cross-sectional design.
PREVALENCE OF ABDOMINAL OBESITY IN NORMAL-BMI INDIVIDUALS
The prevalence of 14.8% aligns with global evidence showing that BMI does not fully capture fat distribution. Studies in Canada19 and the French Constances cohort1,2,4 demonstrate that waist circumference is a stronger predictor of cardiometabolic risk than BMI alone. Our findings reinforce this evidence in a Congolese context, suggesting abdominal obesity among normal-BMI adults is a relevant target for prevention.
The apparent increased risk in men after adjustment (ORa = 5.376) may reflect visceral fat accumulation typical of android fat distribution.19 However, the reversal from crude to adjusted odds ratios suggests possible confounding or model instability. Similarly, the higher risk in adults under 40 years (ORa = 4.945) may indicate early exposure to sedentary behaviors or dietary changes, though these mechanisms remain hypothetical.20–22
DIETARY HABITS
Dietary intake was broadly similar between adults with and without abdominal obesity (Figures 2–3). Staple foods such as cassava, rice, plantain, and chikwangue were consumed by most participants, alongside high intake of vegetables, fruits, and fish. Palm oil use was nearly universal (97.6%). Given the absence of portion size or nutrient composition data, dietary causation cannot be established. Frequency of consumption alone did not differentiate risk.
The reliance on starchy staples and palm oil may contribute to energy-dense diets, but this remains speculative without quantitative dietary assessment. Future studies should measure caloric intake and nutrient profiles to clarify the role of diet in abdominal obesity.18,20–24
FACTORS ASSOCIATED WITH ABDOMINAL OBESITY
Multivariate analysis identified younger age, male sex, smoking, sedentary lifestyle, and hypertension as significant correlates (Table III). Education appeared protective, with secondary and higher education linked to lower odds. This may reflect greater health awareness or access to information, though the study did not directly measure knowledge or behaviors, so the protective role of education remains hypothetical.18,22
Smoking and hypertension were positively associated with abdominal obesity, consistent with evidence that both contribute to metabolic dysregulation.6,19,25 Sedentary lifestyle also emerged as a risk factor, aligning with Haregu et al.26 These associations are biologically plausible and consistent with prior literature, but causality cannot be inferred
STRENGTHS AND LIMITATIONS
This study benefits from a large sample size and standardized measures, enabling exploration of abdominal obesity in normal-BMI adults. Multivariate analysis strengthened validity. However, the cross-sectional design limits causal inference, self-reported behaviors risk bias, dietary data lacked detail, and purposive sampling may affect representativeness. Odds ratio reversals highlight model instability.
CONCLUSION
Abdominal obesity affected 14.8% of normal-BMI adults in Gombe Matadi. Key correlates included smoking, sedentary lifestyle, and hypertension, while education was protective. Findings support waist circumference screening, tailored counseling, and preventive strategies. Longitudinal research is needed to clarify causal pathways and inform context-specific interventions.
ACKNOWLEDGEMENTS
We are grateful to the RIPSEC project managers for their valuable support and guidance, and to the ESPK Ethics Committee for their oversight and approval of this study.
DISCLAIMER
The views expressed in this article are those of the authors and do not necessarily represent the official position of their affiliated institutions.
ETHICS STATEMENT
The ESPK Ethics Committee approved this secondary study (No.ESP/CE/60/2025). Written informed consent was obtained from all participants involved in the study.
DATA AVAILABILITY
The data supporting the findings of this study are available from [insert source or repository]. Publicly available datasets can be accessed at: [insert link]. (Delete if not relevant)
FUNDING
This research received no external funding.
AUTHORSHIP CONTRIBUTIONS
-
Panda AM: Conceptualization, study design, data collection, manuscript drafting.
-
Nkongolo BK: Methodology and statistical analysis of results.
-
Mapatano MA: Literature review, data validation, critical revisions.
-
Muyer MTMC: Supervision, project administration, final approval of the manuscript.
All authors meet the ICMJE criteria for authorship, have read and approved the final manuscript, and agree to be accountable for all aspects of the work.
Disclosure of interest
The authors completed the ICMJE Disclosure of Interest Form (available upon request from the corresponding author) and declare no conflicts of interest.