Exclusive breastfeeding (EBF) is a cornerstone of public health, recognized for its capacity to reduce infant morbidity and mortality. It is defined as feeding an infant only breast milk for the first six months of life, without any additional food or drink except when medically indicated.1 The benefits are well established, including the prevention of more than 510,000 maternal and infant deaths and 4.58 million cases of childhood obesity annually.2 Despite this evidence, global prevalence remains low at 44%, below the WHO target of 50% by 2025.3
In Africa, the average prevalence is 44.3%, with marked regional disparities: 59.1% in East Africa compared to 35.1% in West Africa.4 Breastfeeding practices are shaped by sociodemographic, obstetric, and psychosocial factors such as maternal age, education, parity, antenatal care, and community support.4,5 Persistent barriers include perceptions of insufficient milk supply, inadequate provider training, lack of skilled support, aggressive marketing of substitutes, and limited maternity leave policies.5
In the Democratic Republic of Congo (DRC), 73.4% of infants are breastfed within the first hour of life, and 59.6% are exclusively breastfed.6 Kasai Oriental shows even higher rates, with 85.1% for early initiation and 89.8% for EBF according to PADRIR.7 National surveys also indicate progress, rising from 24% in 2001 to 53.5% in 2018.8 These improvements reflect initiatives led by PRONANUT, including essential family practices, community outreach, cooking demonstrations, and preschool consultations.9 However, SMART surveys continue to highlight a correlation between low adherence to EBF and child malnutrition.
Local studies reveal persistent gaps. For example, research in Bipemba in 2020 reported an EBF prevalence of 45.5%, with 74% of mothers informed and 62.6% supportive of the practice.10 Despite encouraging provincial averages, disparities remain, and no study has yet examined the Lubilanji health zone. This gap is critical, as healthcare providers’ knowledge and counseling are consistently identified as key determinants of maternal adherence to EBF, directly influencing breastfeeding outcomes. Without understanding how well-equipped local providers are to promote and support EBF, strategies risk being ineffective or poorly adapted to community realities.
Therefore, this study focuses on Lubilanji to explore the knowledge, attitudes, and practices of healthcare professionals regarding EBF. By addressing this gap, the research aims to strengthen local strategies, align with national priorities, and contribute to achieving global EBF targets.
METHODS
Type of study
This is a descriptive cross-sectional study of healthcare professionals in health care establishments (HCEs) in the Lubilanji health zone in the province of Kasai Oriental.
Study framework
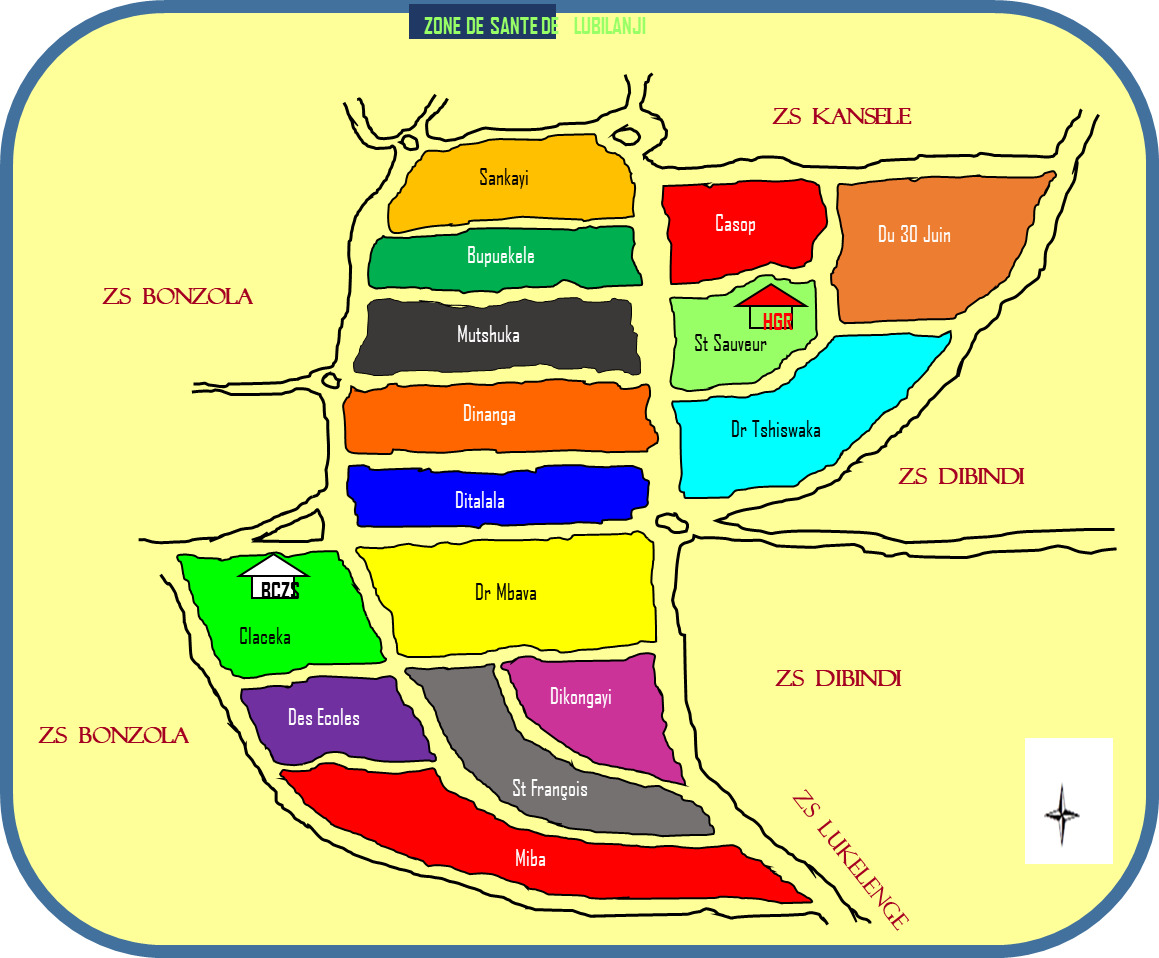
The study took place in the Lubilanji health zone (Kasai Oriental, DRC), covering 16 km² and serving a population of 323,041, including 61,053 children under five (2023). It comprises 36 facilities spread across 15 health areas, with 196 healthcare professionals and 1,912 community health workers, including 166 community health workers. Lubilanji is bordered by Dibindi, Kansele, Bonzola, and Lukelenge. The Dinanga and Ditalala facilities each employ 28 healthcare professionals.
.png)
Study population
The study population consisted of healthcare professionals working in healthcare facilities (HCFs) in the Lubilanji health zone, Kasai Oriental province. The statistical unit was defined as any healthcare professional (physician, nurse, midwife, laboratory technician, etc.) present in the targeted facilities during the survey. Inclusion criteria were informed consent and availability during data collection. Professionals absent or refusing participation were excluded. This ensured representativeness and reliability of the data.
Sampling
The minimum sample size was calculated using the proportion formula with a 95% confidence level (Z = 1.96), precision of 5% (d = 0.05), and estimated prevalence of 89.8% (PADRIR). The result (141) was increased by 10% for nonresponse, yielding 155 participants.
A three-stage probability sampling was applied:
-
Exhaustive selection of the 15 health areas of Lubilanji;
-
Inclusion of all healthcare facilities in each area;
-
Survey of all eligible professionals until the required sample size was reached.
Stratification by health area ensured proportional representation. Nonresponses were replaced within the same stratum. Weighting was unnecessary as distribution was proportional.
Study variables
This cross-sectional descriptive study examined the triad of knowledge, attitudes, and practices (KAP) regarding exclusive breastfeeding (EBF) as the dependent variable. Independent variables included:
-
Socio-demographic: age, education, parity, marital status, residence;
-
Professional: role, department of assignment;
-
Behavioral/institutional: frequency of health education, availability of tools, use of guides, family awareness, nutritional assessment;
-
Contextual: sources of information, family influence, place of birth, level of knowledge.
Composite KAP scores were constructed using 10 items for knowledge, 8 for attitudes, and 7 for practices. Each correct/positive response scored one point. Scores were categorized as “excellent” (≥80%), “good” (60–79%), “average” (40–59%), or “poor” (<40%), ensuring transparency and reproducibility.
Data collection
Data were collected through face-to-face interviews using a SurveyCTO questionnaire via KoboCollect on Android devices. The protocol was validated by the thesis supervisor and approved by the Ethics Committee of the School of Public Health, UNIKIN. Six trained interviewers conducted the survey after a two-day training and pre-test in Mbuji-Mayi. The two best were appointed supervisors. Each interviewer completed about 26 interviews over five days, with oversight from the principal investigator.
Data processing and analysis
Daily checks ensured completeness and consistency. Data were exported from Kobo to Excel and analyzed with SPSS version 26. Qualitative variables were presented as frequencies, quantitative variables as mean ± SD or median with IQR. Composite KAP scores were analyzed descriptively and inferentially to explore associations with socio-demographic and professional variables.
Ethical considerations
The study adhered to UNIKIN ethical standards of respect, beneficence, and justice. Informed consent was obtained, participation was voluntary, and confidentiality was guaranteed. Competency scoring criteria were explicitly defined, and data were coded to preserve anonymity.
RESULTS
Sociodemographic characteristics of healthcare professionals
Table 1 and Table 2 summarize the respondents’ profiles. Most healthcare professionals were aged 33–42 years (mean 34.9), married (90%), and held higher education (55%). Religious affiliations were diverse, with Pentecostal (36%) and Catholic (30%) churches most represented. Professionally, nurses constituted the largest group (60%), followed by midwives (26%) and physicians (7%). More than half (54%) resided outside the Lubilanji health zone despite working within it, suggesting commuting patterns may affect continuity of care and breastfeeding counseling. Half of respondents were multiparous, and 59% reported their youngest child was older than 13 months, indicating personal breastfeeding experience alongside professional knowledge.
Knowledge about EBF
Almost all respondents (99%) reported prior information on EBF (Table 3). Healthcare staff were the main source (83%), followed by schools (65%) and radio (36%). Knowledge levels varied (Table 4): 50% had average knowledge, 27% excellent, 15% superior, and 6% poor. This highlights that while awareness is nearly universal, depth of understanding remains uneven.
Attitudes towards EBF
Most respondents (71%) strongly agreed that infants should be exclusively breastfed for six months (Table 5), with 19% agreeing and 10% disagreeing. The perception that fathers feel abandoned was largely rejected (94%). Attitudes toward bottle-feeding were divided: 51% considered it practical for working mothers, while 48% disagreed. Similarly, 75% rejected the idea that bottle-feeding is more practical than EBF. Overall, 48% of attitudes were rated very good or good, 27% fairly good, and 25% poor. These findings suggest strong theoretical support for EBF but persistent doubts about feasibility in the context of maternal employment.
Practices related to EBF
In practice (Table 6), 43% of healthcare professionals demonstrated very good EBF practices, 25% fairly good, and 32% poor. No respondent was classified as “good,” reflecting polarization between strong adherence and weak implementation. Professionally (Table 7), physicians had higher knowledge scores (36% excellent) but less favorable attitudes, while nurses and midwives, though less knowledgeable, reported stronger attitudes and greater practical engagement. This divergence indicates that professional role influences both promotion and practice of EBF.
DISCUSSION
Keys results
This study, conducted with 155 healthcare professionals in the Lubilanji health zone, assessed their knowledge, attitudes, and practices (KAP) regarding exclusive breastfeeding (EBF). Respondents were predominantly aged 33–42, married (90%), and highly educated (55%). Nurses formed the majority (60%), and more than half resided outside the health zone (54%). Nearly all participants (99%) had prior information on EBF, mainly from healthcare staff (83%). While 27% demonstrated excellent knowledge, half showed only average knowledge. Attitudes were favorable among 71%, though 25% expressed reservations. Practices were polarized, with 43% rated very good and 32% poor. Physicians displayed stronger knowledge but less favorable attitudes compared to nurses and midwives.
Findings in the context of the literature
Almost all respondents had prior exposure to EBF information, primarily through prenatal and preschool consultations. These findings align with Sidibé AK et al.5 and Sacko et al.,11 but differ from Coulibaly, who reported only 61.6% of professionals informed.12 The most cited benefits were protection against infections (85%) and healthy growth (50%), higher than Sidibé AK et al. (38.6% and 19.5%),5 but different from Berthe, who emphasized healthy growth (74.2%) and birth spacing (2.4%).13
Despite high awareness, knowledge depth was uneven. This suggests that dissemination alone does not ensure comprehensive understanding. Limited continuing education, outdated materials, and insufficient counseling training may explain this gap. Structured refresher programs and standardized guidelines are needed to strengthen professional knowledge and ensure it is actionable.
Most respondents (71%) supported EBF up to six months, a higher rate than reported by Abdulwali Sabo et al. in Nigeria (23%).11 This difference may reflect stronger local awareness or provider commitment. Interestingly, 47% rejected the idea that fathers feel excluded, contrasting with Muya’s findings in Mbuji-Mayi,10 suggesting evolving family perceptions in Lubilanji.
The paradox of physicians showing stronger knowledge but weaker attitudes may be explained by workload priorities. Physicians often focus on curative care, leaving less time for preventive counseling, while nurses and midwives are more engaged in maternal and child health services, making them more attuned to breastfeeding realities. Professional role and workflow constraints therefore shape attitudes.
Regarding working mothers, 39% considered bottle-feeding acceptable, though 77% rejected it as less practical than breast milk. This contrasts with Nigerian findings.11 Importantly, expressed breast milk was not widely considered as a strategy to reconcile employment with continued EBF. Future interventions should emphasize this option to support working mothers. Religious diversity also influenced attitudes, with 36% of respondents belonging to Pentecostal churches, differing from Coulibaly’s study in Mali, where 99% were Muslim.12
Early initiation was common (74%), higher than Coulibaly (62.6%),12 Sacko et al. (28.7%),14 and Berthe (26%).15 This reflects professional awareness and alignment with recommendations. However, only 48% practiced breastfeeding on demand, similar to Sacko14 but lower than Sidibé and Sékou.16,17 All respondents acknowledged colostrum’s importance, consistent with Sidibé16 and Sékou.17
The discrepancy between strong initiation and weaker sustained practices highlights systemic barriers. Healthcare professionals may struggle to balance professional duties with on-demand feeding. Cultural traditions, such as giving water before six months (46%), persist despite awareness of best practices. Institutional support and cultural change are therefore essential.
Parity also influenced practices: first-time mothers tended to adhere more consistently to recommended behaviors, while multiparous women were more likely to adopt alternative feeding approaches. This difference underscores the need for parity-sensitive counseling strategies.
Overall, 43% of respondents had very good practices, 25% fairly good, and 32% poor. These results are lower than Takassi in Togo (51.8%)18 and Gueye in Senegal (67.42%),19 but higher than Sabo and Abba,11 reflecting contextual differences in engagement.
Strengths and weaknesses
The study’s strength lies in its exclusive focus on healthcare professionals, ensuring expertise and representativeness through diverse sampling. However, systemic weaknesses were evident, including limited continuing education, lack of educational materials, and inadequate workplace frameworks to support breastfeeding. These constraints likely explain why strong knowledge did not consistently translate into favorable attitudes or effective practices. Addressing these barriers through structured training, provision of counseling tools, and workplace adaptations is essential to strengthen exclusive breastfeeding promotion and ensure that professional knowledge is effectively applied in practice.
CONCLUSIONS
This study in the Lubilanji health zone revealed that physicians demonstrated stronger knowledge of maternal and child health principles but held less favorable attitudes toward exclusive breastfeeding compared to midwives, who adhered more closely, and nurses, whose practices were constrained by workload and institutional barriers. Despite high awareness, uneven practices highlighted gaps in counseling skills, educational tools, and system-level support. Physicians’ weaker attitudes despite stronger knowledge suggest that professional roles and workflow priorities shape engagement with breastfeeding promotion. The absence of materials and dedicated counseling spaces further undermined effective practice. Recommendations include structured continuing education, provision of practical counseling resources, workplace adaptations, and culturally tailored awareness activities to ensure knowledge translates into consistent practice.
ACKNOWLEDGEMENTS
We are grateful to all the healthcare professionals who participated in this study, as well as the heads of the health facilities in the Lubilanji health zone for their collaboration and availability.
DISCLAIMER
The opinions expressed in this manuscript are those of the authors and do not necessarily reflect those of associated health or academic institutions.
ETHICS STATEMENT
This study was approved by the Ethics Committee of the Kinshasa School of Public Health (approval number: CE/ESP/2025/042). Informed consent was obtained from all participants before their inclusion in the study.
DATA AVAILABILITY
The data used for this research are available from the lead author upon reasoned request. They are not publicly accessible in order to protect the confidentiality of the participants.
FUNDING
This research received no external funding. The costs associated with publishing this article were not covered by any third-party source.
AUTHORSHIP CONTRIBUTIONS
KAPINGA TSHIBALA Marlène: lead author, study design, data collection and analysis, manuscript writing.
Nkongolo Bernard-Kennedy: contribution to the writing and critical review of the manuscript.
Kalonji Moise: contribution to the writing and critical review of the manuscript.
Tshisuaka Basile: contribution to the writing and critical review of the manuscript.
Jean Nyandwe Kyloka: field facilitator, supervision, and approval of the protocol and manuscript.
DISCLOSURE OF INTEREST
The authors completed the ICMJE Disclosure of Interest Form (available upon request from the corresponding author) and disclose no relevant interests.