Introduction
Scientific literature continues to grow exponentially, doubling approximately every twelve to fifteen years.1 This pattern is evident across health disciplines and regions. Studies across high-income countries consistently demonstrate limited health literacy among the general population, with only 12% of US adults demonstrating proficient health literacy, and similar patterns observed across Europe.2,3 While health literacy measurements vary across contexts and tools, studies from low- and middle-income countries (LMICs) reveal similar challenges, with additional barriers of limited educational access, linguistic diversity, and resource constraints compounding difficulties in accessing and applying research evidence.4–6 Simultaneously, public trust in scientific institutions has declined in several contexts, particularly around contentious health topics.7 This disconnect between expanding evidence bases and limited public access to usable health information undermines research investment value and weakens evidence-informed policy, with the gap between research production and practical application widest in regions that could benefit most from evidence-based interventions.
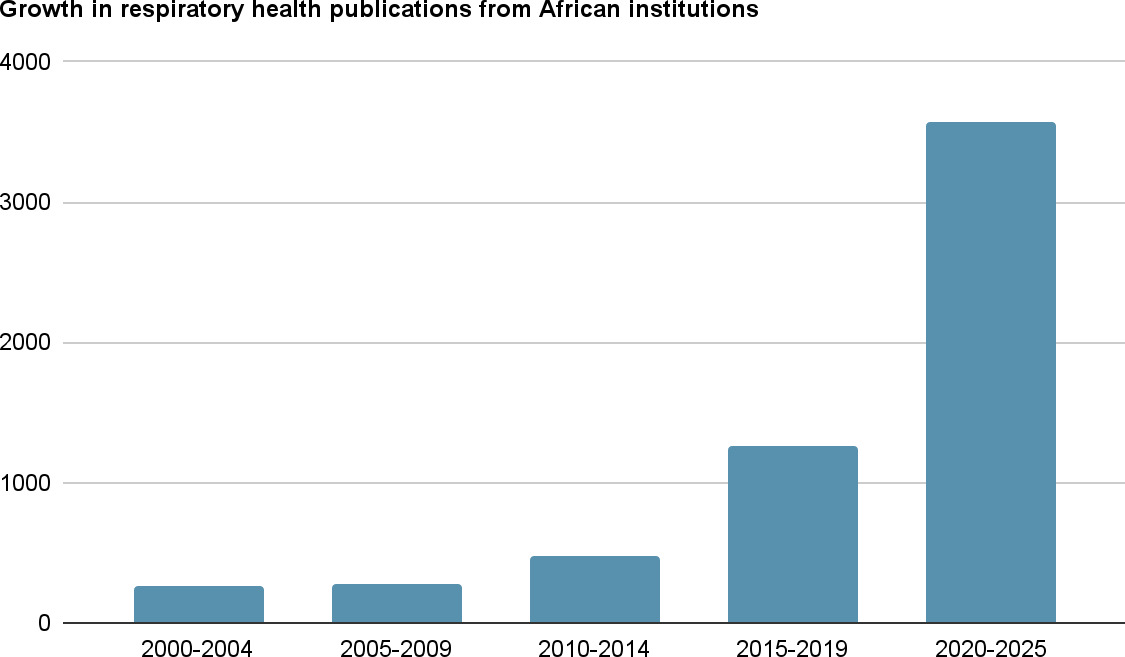
Using respiratory health outputs from African-affiliated institutions, for example, PubMed-indexed publications increased fourteen-fold from 257 in 2000-2004 to 3,575 in 2020-2025 (Figure 1), with growth accelerating markedly after 2015. Yet this proliferation has not translated into improved public understanding or equitable access to research-informed health information, with consequences most severe in resource-constrained settings.

This viewpoint examines factors contributing to this gap and argues for co-produced, multi-format approaches to research communication. The paper further explores economic and policy implications of knowledge translation gaps and the incorporation of relevant translation strategies within essential health infrastructure, particularly in low- and middle-income countries (LMICs).
The paradox of proliferation: more research, less clarity
The past two decades have witnessed unprecedented growth in health research publications. For example, a PubMed search using the terms “health research” OR “public health” over the period 2000-2024 yields 379,808 publications, with output accelerating significantly in recent years. While this reflects scientific progress, it has paradoxically created accessibility challenges even within academia.
Systematic reviews and meta-analyses have become essential precisely because individual researchers cannot comprehensively interpret rapidly expanding evidence bases. Ioannidis argues that systematic reviews have proliferated not only due to volume but also because of redundancy and methodological inconsistencies across primary studies, creating “research waste”.8 Yet even systematic reviews frequently present inconclusive or conflicting findings, often hedged with statistical caveats and methodological qualifications that lay audiences struggle to interpret. Without translation into simple, usable, and adaptable formats that contextualise findings for practical application, even synthesised evidence remains largely inaccessible to the public and fails to inform everyday health decisions. If trained researchers require structured synthesis tools to navigate evidence, populations without specialist training face exponentially greater barriers in accessing and applying research to improve their health.
Research methods have grown increasingly sophisticated, employing advanced statistical techniques and complex study designs. While methodological rigour is essential, it creates communication challenges when findings must be translated for non-specialist audiences. The very features that make research credible: statistical nuance, careful qualification of claims, and acknowledgement of limitations, become obstacles to public comprehension9
Why research fails to reach the public
Linguistic and structural barriers. Academic research uses discipline-specific terminology, statistical jargon, and methodological conventions, creating significant comprehension barriers. Health literacy research demonstrates that even educated populations struggle to interpret research findings, particularly statistical concepts such as relative versus absolute risk, confidence intervals, and effect sizes.10,11 Schwartz et al. found fewer than 20% of physicians correctly interpreted basic screening statistics.12 Research articles follow structural conventions optimised for peer review rather than public understanding, reflecting what might be termed “academic elitism” - a culture where complex language and technical presentation are valued as markers of scholarly status, with simplified communication sometimes perceived as less rigorous or less prestigious. Even “simplified” abstracts often retain technical complexity.13
Misaligned incentive structures. Academic reward systems prioritise publication volume, citation metrics, and grant acquisition over public engagement.14 Promotion criteria emphasise research outputs measurable through bibliometrics rather than societal impact or knowledge translation activities.14 Consequently, researchers receive limited training in science communication, and engagement work remains undervalued. This structural misalignment is not researcher disinterest; surveys show scientists express willingness to engage publicly but cite time constraints, lack of institutional support, and concerns about misrepresentation as barriers.15 The problem is systemic, not individual.
Access barriers and inequalities. Paywalls restrict access to primary research, with a large share of recent scientific articles remaining behind publisher paywalls despite open-access initiatives.16 However, open access initiatives themselves often perpetuate inequalities. Many OA models rely on article processing charges (APCs) that can range from $1,500 to $5,000 per publication,17 costs that are prohibitively expensive for researchers in LMICs, where such fees may represent months or years of research budgets. While some publishers offer fee waivers or discounts for LMIC authors, these programs are inconsistently applied, bureaucratically complex to access, and inadequately publicised.18 Moreover, transformative agreements and institutional OA partnerships are predominantly concentrated in high-income countries, creating a two-tier system where researchers in well-resourced institutions can publish openly while LMIC researchers face barriers to both accessing and contributing to the open scientific literature.16
Populations most affected by health inequities, those with lower educational attainment, limited digital literacy, or speaking languages other than English, face compounded barriers. The dominance of English in scientific publishing marginalises non-English speakers, while research often fails to reflect diverse cultural contexts.19 These inequalities create a troubling pattern: those who could benefit most from research-informed health decisions have the least access to credible evidence. Furthermore, researchers from high-income countries frequently lead research grants focused on LMICs without appropriate or equal involvement of LMIC-based researchers who are best positioned to understand local contexts. This results in findings that may not reflect population needs or priorities.20 While initiatives promoting North-South research collaboration exist, including capacity-building programs and equitable partnership frameworks, these remain inadequate in scale and often reproduce power imbalances in research leadership, funding allocation, and authorship.19
Media dynamics and misinformation. Contemporary information ecosystems amplify sensational, emotionally charged, or misleading content over careful scientific evidence.21 Research examining health misinformation identifies multiple contributing factors: political polarisation, media preference for novelty over nuance, algorithmic amplification of engaging content, and spread of inaccurate information through social media.22,23 Southwell and colleagues demonstrate that corrections and fact-checking, while somewhat effective, struggle to overcome initial misinformation exposure, particularly when false information aligns with pre-existing beliefs.24 Evidence-based findings must compete for attention against content optimised for engagement rather than accuracy.
Evidence from knowledge translation research
Research across multiple health contexts demonstrates that evidence does not automatically translate into improved understanding or health outcomes. Knowledge translation frameworks, such as Graham et al.'s Knowledge-to-Action cycle, emphasise that moving research into practice requires deliberate, structured processes including knowledge synthesis, stakeholder engagement, implementation strategies, and outcome evaluation.25
Embedded research models, where researchers work directly alongside practitioners and communities, have shown promise. Akintola et al. describe case studies where embedded researchers co-produced knowledge with stakeholders, resulting in contextually relevant research translated into actionable practice.26 Evidence examining plain language communication shows promising but mixed results.13 Protheroe et al.'s systematic review found plain language health information can improve comprehension, though effects vary by intervention design.27 Importantly, studies demonstrate that plain language health materials can maintain scientific accuracy while improving readability when developed through iterative testing with target audiences and review by content experts, challenging the assumption that accessibility necessarily compromises rigour.28
However, existing knowledge translation efforts, including Cochrane Plain Language Summaries, NHS Behind the Headlines, and The Conversation, while valuable, have not achieved widespread population reach.29 For example, Cochrane summaries are accessed primarily by health professionals rather than the general public.30 This suggests that the availability of simplified information, while necessary, is insufficient without strategies that address discoverability, engagement, and multi-format dissemination.
Toward integrated knowledge translation approaches
Key principles
Addressing the research-public awareness gap requires recognising research translation as essential health infrastructure. Drawing on knowledge translation frameworks, specifically Graham et al.'s Knowledge-to-Action cycle25 and Straus et al.'s integrated knowledge translation model,31 and evidence from communication science, including the Elaboration Likelihood Model and health belief frameworks,32 several principles emerge:
First, co-production of knowledge with communities, practitioners, policymakers, and communication specialists ensures research addresses relevant questions and generates actionable findings. Co-production is genuinely collaborative knowledge creation where diverse expertise shapes research from inception.33 For example, the CanTest Collaborative in the UK involves patients, primary care practitioners, and researchers in co-designing cancer diagnostic research, resulting in studies that address real-world clinical uncertainties and produce findings directly applicable to practice.34
Second, multi-format dissemination recognises that different audiences require different formats. Evidence briefs serve policymakers; plain language summaries support patients; visual infographics engage social media audiences; animations explain complex methods. No single format suffices.35 The COVID-19 pandemic demonstrated this principle’s importance: public health agencies that deployed multi-format communication, including video explainers, infographics, plain language fact sheets, and social media content, achieved significantly higher public reach and comprehension than those relying solely on written reports.36 The Cochrane Collaboration’s expansion from technical summaries to plain language summaries, video abstracts, and visual abstracts similarly increased accessibility across diverse user groups.30
Third, evidence-informed communication frameworks balance accessibility with accuracy. Research demonstrates that clarity need not sacrifice nuance when communicators understand both content and audience.37 However, this requires training; most researchers lack formal instruction in public engagement. Structured science communication training programs have shown that researchers can improve their ability to explain complex concepts accessibly without oversimplification, with participants demonstrating measurable improvements in public engagement effectiveness.38
Fourth, embedding communication within research design rather than relegating it to post-publication dissemination ensures translation is planned, resourced, and evaluated. Several funding agencies now require knowledge translation plans, though implementation remains inconsistent.39 The Canadian Institutes of Health Research (CIHR) integrated knowledge translation approach, which mandates stakeholder engagement from study conception, has demonstrated that early communication planning leads to faster research uptake and broader impact compared to post-hoc dissemination efforts.40 Similarly, the UK’s National Institute for Health Research (NIHR) requires applicants to detail public involvement and dissemination strategies at the grant application stage, resulting in more targeted and effective knowledge mobilisation.
Fifth, digital tools and platforms can support scalable, context-sensitive translation. While technology alone cannot solve structural problems, well-designed digital infrastructure can reduce barriers. Knowledge brokering approaches, which organise interactive processes between knowledge producers and users to co-produce feasible and research-informed options, demonstrate the potential of intermediary mechanisms to strengthen the relationship between research and policy communities.41
However, implementing these principles faces challenges observed across multiple contexts. For example, funding remains a persistent barrier, with communication activities often treated as “add-ons” rather than core research components, limiting resource allocation for professional communication support, multi-format content development, or evaluation of translation effectiveness.
There are also legitimate concerns about oversimplification when complex findings are reduced to summaries, tensions evident in stakeholder consultations where researchers worried that accessible language might be misinterpreted or lack necessary caveats. Moreover, who should conduct translation work remains contested. Some argue researchers bear responsibility for communicating their findings; others suggest science communication should be professionalised with trained intermediaries. Evidence from successful initiatives suggests both approaches are needed: researchers must engage more actively in translation, while also collaborating with communication specialists who bring complementary expertise in audience analysis, message design, and multi-platform dissemination. The most effective models observed involve interdisciplinary teams where researchers provide content expertise and communication professionals provide translation expertise, as demonstrated in projects like the C2REST study, where dedicated communication support enabled more effective and sustained public engagement than researcher-led efforts alone.
Digital platforms as translation infrastructure: possibilities and limitations
Digital technologies offer opportunities to scale research translation while maintaining quality. Platforms integrating plain language generation, visual data representation, multi-format outputs, and crowdsourced validation could potentially support more efficient knowledge mobilisation. Such platforms might enable researchers to upload manuscripts and receive suggested summaries, infographics, or video scripts, with validation mechanisms ensuring accuracy through multi-stakeholder review.
However, several caveats apply. No technological solution can substitute for fundamental changes in incentive structures, funding priorities, and institutional cultures that currently undervalue translation work. Automated or semi-automated translation risks oversimplification if not carefully designed and validated. Digital platforms may inadvertently widen inequalities if they primarily serve already-engaged, digitally literate audiences while failing to reach marginalised populations.
Existing digital tools, including automated summarisation algorithms and AI-powered translation services, demonstrate both promise and limitations. Studies examining their accuracy reveal inconsistent performance, particularly for complex health information requiring contextual interpretation.42 This suggests effective platforms would likely require human-AI collaboration rather than full automation. Consequently, developing robust, validated, and equitable digital translation infrastructure represents a critical priority for research and innovation to ensure accessible, accurate research communication reaches diverse populations and informs evidence-based decision-making.
Implications for global health policy and economics
Economic and policy consequences
The gap between scientific production and public understanding generates significant economic and policy consequences, with disproportionate impacts in low- and middle-income countries (LMICs) where resource constraints compound translation challenges.
Diminished returns on research investment occur when findings remain siloed within academic communities. Chalmers and colleagues estimate that up to 85% of research investment may be wasted through avoidable inefficiencies, including inadequate dissemination and uptake.43 When research findings fail to reach policymakers, practitioners, or communities, the economic opportunity cost is substantial, representing foregone health improvements, inefficient resource allocation, and missed opportunities for evidence-informed policy. From a health economics perspective, ineffective research translation represents market failure. Research is a public good, yet information asymmetries and coordination failures prevent optimal dissemination. In LMICs, where health research budgets are already constrained, such waste represents particularly significant foregone opportunities, as limited resources produce findings that fail to inform practice or policy.
Weak policy translation has direct economic implications, especially in resource-constrained settings. Oliver et al. identify systematic obstacles preventing policymakers from efficiently accessing research, including a lack of time to review primary literature, insufficient synthesis into policy-relevant formats, and misalignment between research timelines and policy decision cycles.44 These barriers result in policy decisions made without available evidence, potentially leading to ineffective interventions and wasted resources. In LMICs, where evidence-informed policymaking could optimise limited health system resources, translation gaps perpetuate inefficiencies and missed opportunities for cost-effective interventions.
Trust erosion, misinformation, and health inequities compound these economic consequences. Trust erosion in scientific institutions occurs when research is misunderstood, inconsistently communicated, or perceived as disconnected from community concerns. Declining trust complicates public health responses, as evidenced by communication challenges during the COVID-19 pandemic.45 Increased susceptibility to misinformation follows from limited access to credible evidence.46 Widening health inequities result when those with higher health literacy disproportionately benefit from research advances.47 The costs of limited health literacy extend beyond health outcomes to include economic burdens on health systems and reduced productivity.48 In LMICs, where health systems already face capacity constraints, these compounded consequences widen existing gaps between populations and regions.
Priorities for low- and middle-income countries
Strengthening research translation infrastructure holds particular importance for global health, where evidence-informed decision-making is critical yet information inequalities intersect with resource constraints. In LMICs, limited access to research, both due to paywalls and lack of contextually relevant evidence, compounds challenges facing health systems.49
Improved research translation in LMIC contexts could: support evidence-informed policymaking where decision-makers lack time to review primary research; maximise limited health research budgets through efficient knowledge mobilisation; enhance community engagement in health programmes by making findings accessible; facilitate South-South knowledge exchange and regional learning; reduce misinformation by providing accessible credible alternatives; support capacity building for local researchers and policymakers; improve health literacy as part of health system strengthening; and ensure locally relevant evidence informs context-appropriate interventions.
In resource-constrained health systems, maximising returns on research investment is essential. Improved translation infrastructure could enhance allocative efficiency by ensuring policymakers have access to relevant evidence when making resource allocation decisions. For example, accessible summaries of cost-effectiveness analyses could inform procurement decisions, plain language guidelines could support frontline health worker training, and multi-format dissemination could enable community health programs to integrate evidence-based practices.
Strengthening research translation requires policy interventions across multiple levels, with particular attention to LMIC contexts. Funding agencies can mandate knowledge translation plans with dedicated budgets, recognising that LMICs may require additional support for translation activities. Universities can reform promotion criteria to value translation activities alongside traditional research outputs, acknowledging that communication to local policymakers and communities represents meaningful impact. Health systems can establish knowledge broker roles connecting researchers with decision-makers, as demonstrated by successful intermediary organisations in some African and Asian contexts.43 Regulatory frameworks can incentivise open access publishing and reduce financial barriers for LMIC researchers to publish their findings openly.
However, realising these benefits requires investment, coordination, and commitment to equity. Translation efforts must be culturally appropriate, linguistically accessible, and responsive to community-identified priorities rather than imposing external frameworks. This necessitates genuine partnerships between researchers in high-income countries and LMICs, with resources directed toward building local capacity for research communication rather than simply disseminating Northern-produced evidence.50 Capacity building should include training LMIC researchers in communication skills, supporting development of regional knowledge translation networks, investing in local language translation and culturally adapted materials, and ensuring LMIC voices lead in defining translation priorities and approaches for their contexts.
Conclusions
The gap between scientific output and public understanding is widening. Despite unprecedented research production, health literacy remains limited, misinformation persists, and populations most affected by health inequities face the greatest barriers to accessing credible evidence. This disconnect undermines the societal value of scientific investment, threatens public trust in research institutions, and results in substantial economic waste through foregone health improvements and inefficient resource allocation. Addressing this challenge requires recognising research translation as essential infrastructure, not an optional afterthought. Evidence from knowledge translation frameworks, health economics, and communication science points toward integrated approaches combining co-production, multi-format dissemination, evidence-informed communication design, and sustained investment in translation capacity.
Digital platforms may offer scalable solutions, though they cannot substitute for fundamental structural changes in how research is valued, funded, and conducted. Critically, translation efforts must prioritise equity, ensuring that accessibility improvements reach populations currently excluded rather than primarily benefiting already-engaged audiences. The research community faces a choice: continue producing evidence that remains inaccessible to most who could benefit, or commit to a transformation that positions understanding as central to scientific enterprise. The latter path requires acknowledging that research excellence is measured not only by methodological rigour or publication impact, but by whether knowledge reaches and benefits the communities it aims to serve. Building research translation infrastructure is feasible, evidence-informed, and essential for maximising returns on public research investment and strengthening evidence-informed health policy. The question is whether the scientific community will prioritise it.
Funding
None declared
Competing interests
The author is developing a digital research translation platform as part of ongoing research, though no commercial interests exist at present.
Author contributions
SO is the sole author.
Acknowledgements
The author thanks colleagues at Teesside University for the discussions that informed this work.