Alcohol consumption is a major public health problem due to its numerous medical, social and economic consequences .1 Among adolescents and young adults, alcohol is often perceived as a mood enhancer, increasing self-confidence and facilitating social interactions.2
Globally, the harmful use of alcohol is a causal factor in more than 200 diseases and injuries, resulting in approximately 3 million deaths per year, or 5.3% of global mortality, including 1.5 million deaths among adolescents and young adults aged 10 - 24 years.3 The intoxicating effects of alcohol can also promote risky behaviors, such as unprotected sex.4
In Africa, alcohol consumption is increasing significantly, with prevalence among adolescents and young adults estimated at 22.8%.5 In the Democratic Republic of Congo (DRC), the National Program to Combat Drug Addiction and Toxic Substances (PNLCT/NPFDT) reported that 3% of children aged 10 - 19 consume alcohol.6 Several studies conducted in Kinshasa and other DRC provinces indicate that adolescents and young adults often consume alcohol without concern, thus exposing themselves to risky behaviors. In Kinshasa, alcohol consumption among this population was estimated at 67.3% in 2010.7 Multiple factors can contribute to excessive alcohol consumption among adolescents and young adults, including economic development, culture, social norms, alcohol availability, and the implementation and enforcement of alcohol policies. Individual factors such as age, gender, family situation, and socioeconomic status also play a role.2 For Kayembe (2010), being male, having never attended school, not living with both parents, not having a religious affiliation, and engaging in income-generating activities are associated with higher alcohol consumption among adolescents and young adults.7
Despite regional strategies aimed at preventing or reducing the harmful use of alcohol in Africa,8 the number of adolescents and young people who consume alcohol continues to increase, and Kinshasa remains affected. Given the high prevalence of alcohol consumption among adolescents and young adults in Kinshasa, we selected two HZ based on their geographical characteristics, including the urban Limete HZ and the urban-rural N’sele HZ; but also considering the HIV prevalence in these areas which would be due to alcohol consumption.
METHODS
The study was conducted in Limete and N’sele HZ. The minimum sample size was calculated using the following formula: Where n is the minimum size; z = 1.96, the 95% confidence interval; p, the proportion of adolescents who have already consumed alcohol (67.3%); q, the proportion of adolescents who have never consumed alcohol (q= 100%-p); and d, the desired absolute precision (0.05). The minimum sample size was 338 participants and after accounting for a 10% non-response rate, the final minimum sample size was 372 participants.
-
Sampling: The two HZs, Limete and N’sele were selected using non-probability sampling. This choice was operated according to the 2023 annual report of the Kinshasa Provincial Health Division of all HIV cases detected during that year. All Kinshasa HZs were categorized into two groups, urban and urban-rural HZs. Thus, Limete HZ had detected 1,212 HIV cases (9.3%) for urban HZs, and N’sele HZ, 1,951 cases, (31.2%) for urban-rural HZs. The sample was divided into two equal parts, 186 adolescents and young adults per HZ. Three Health areas, three avenues and households were selected in a simple random manner.
A household survey was conducted on each selected avenue. Households with one or more adolescents or young adults aged 15 - 24 were identified. In each selected household, a single participant was randomly selected.
-
Variables of interest: Alcohol consumption was considered as the dependent variable. According to the literature review, the independent variables included age, sex, school attendance, religion, and having income-generating activities (IGA).
-
Data Collection: Data were collected using Kobocollect software through face-to-face interviews between trained interviewers and participating adolescents or young adults.
-
Data Analysis: The collected data were first exported to Excel and then imported into SPSS version 25 for statistical analysis. Quantitative variables with a normal distribution, such as age at last birthday, were summarized using the median and its IQR. Categorical variables, including sex, activity level, education level, religion, cohabitation, alcohol consumption, location of consumption, and type of alcohol consumed, were summarized as frequencies and proportions with their 95% confidence intervals. Bivariate and multivariate logistic regression analyses were performed to assess the associations between alcohol consumption (dependent variable) and the independent variables. Odds ratios (ORs) and their 95% confidence intervals were calculated to quantify these associations.
-
Ethical considerations: The study protocol was approved by the Ethics Committee of the Kinshasa School of Public Health (approval number: ESP/CE/119/2024). The study adhered to fundamental ethical principles. Participation was voluntary, and confidentiality and anonymity were guaranteed. Written informed consent was obtained from each participant before data collection. For participants under 18 years of age, parental or guardian consent was also obtained.
RESULTS
SOCIODEMOGRAPHIC CHARACTERISTICS OF ADOLESCENTS AND YOUNG ADULTS AGED 15 - 24 YEARS
Of the 372 adolescents and young adults interviewed, more than half were girls. The median age was 17.5 years (IQR: 4 years). Half of the adolescents were between 15 and 17 years old. Most adolescents and young adults were enrolled in school. One-third of adolescents and young adults had income-generating activities. Nearly half attended revivalist churches, and approximately 45.2% lived with both parents. (Table 1)
PREVALENCE OF ALCOHOL CONSUMPTION AMONG ADOLESCENTS AND YOUNG ADULTS AGED 15 - 24 YEARS
Nearly half of the adolescents and young adults interviewed reported having consumed alcohol at least once in their lives. Compared to the N’sele health zone, the Limete health zone had a significantly higher prevalence of alcohol consumption among adolescents and young adults (54.8%; p < 0.038). Among adolescents and young adults, six out of ten reported having consumed alcohol in the past 12 months, with 67.6% reporting this in the Limete health zone. Furthermore, nearly half reported continuing to consume alcohol up to the time of the survey (Table 2).
The mean age of first alcohol consumption was 7.4 ± 2.7 years, and this alcohol consumption was accidental in childhood. Compared to young adults, adolescents were more likely to report having consumed alcohol in their lifetime (Table 3).
TYPE OF ALCOHOL, PLACE OF CONSUMPTION, REASONS FOR CONSUMPTION, FREQUENCY, AND QUANTITY CONSUMED
Beer was the most consumed alcoholic beverage during the first alcohol-drinking experience. Four out of ten adolescents and young adults had their first experience drinking alcohol in a bar or restaurant, while very few reported having their first experience drinking alcohol in a nightclub (0.5%). Approximately seven out of ten adolescents and young adults drank alcohol with friends or peers. Regarding motivation, four out of ten adolescents and young adults reported drinking alcohol out of thirst or craving, while three out of ten drank alcohol to imitate others (Table 4).
Over the past 12 months, beer remained the most consumed alcoholic beverage (59.8%), followed by whisky (21.8%). Regarding frequency of consumption over the past 12 months, four out of ten adolescents and young adults reported drinking alcohol several times a week, while three out of ten reported drinking only occasionally (Table 5).
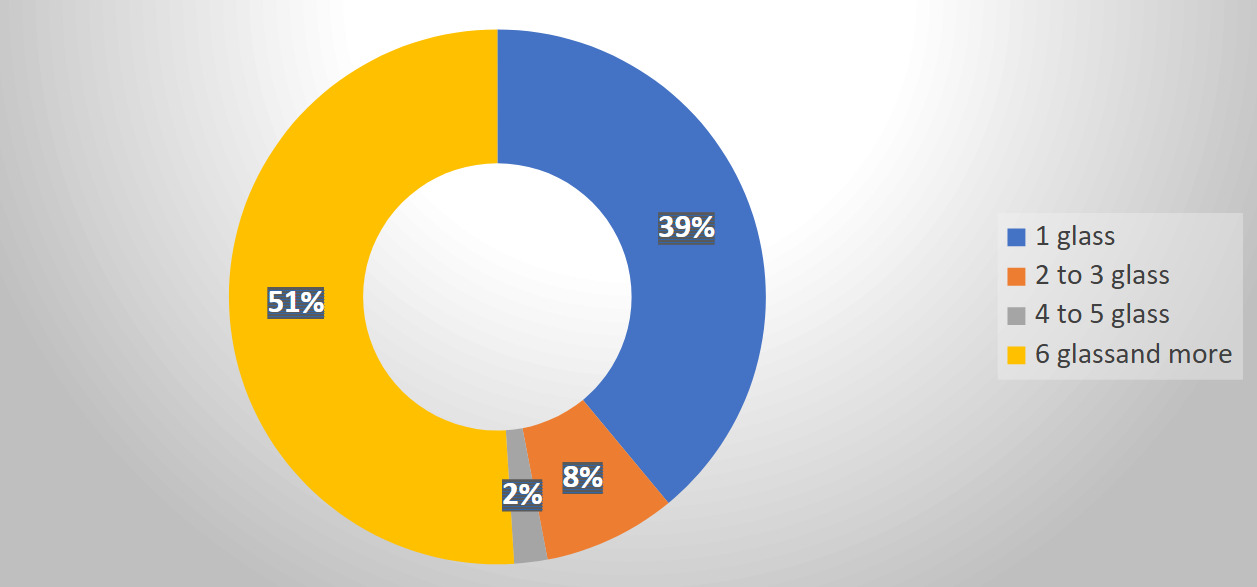
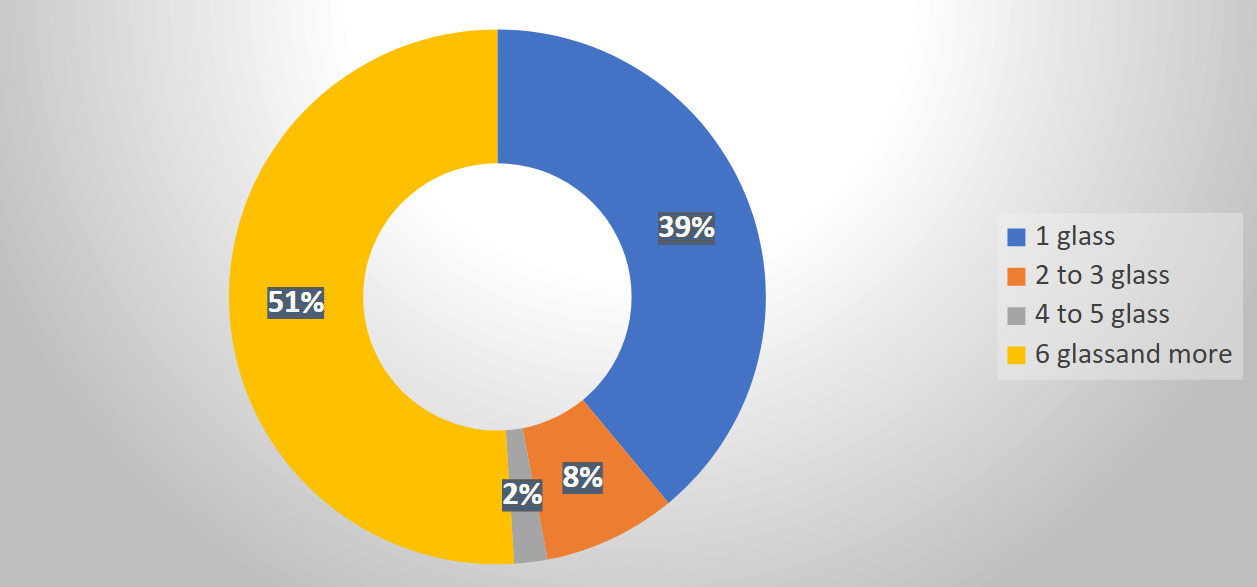
Nearly half of the adolescents and young adults reported consuming six or more alcoholic drinks on a single occasion, compared to four out of ten who reported consuming only one alcoholic drink (Figure 1).
FACTORS ASSOCIATED WITH ALCOHOL CONSUMPTION AMONG ADOLESCENTS AND YOUNG ADULTS AGED 15 - 24 YEARS
Multivariate analyses showed that having an income-generating activity (IGA) OR=3.26 (95% IC= 2.04 to 5.20), p<0.001) was associated with alcohol consumption among adolescents and young adults. Adolescents and young adults with an IGA were 3.26 times more likely to consume alcohol than those without one. (Table 6)
DISCUSSION
The results of this study revealed that nearly half (49.5%) of adolescents and young adults had consumed alcohol at least once in their lives. This prevalence is higher than that reported in Burkina Faso, where 34.14% of students reported having consumed alcohol.9 This difference may be explained by the regulatory environment of schools, which can limit alcohol consumption. Conversely, our prevalence is lower than that observed in Kenge among young motorcycle taxi drivers, where alcohol consumption reached 85,0%.10 Although both groups were adolescents and young adults, the profession of motorcycle taxi driver is an income-generating activity, and alcohol consumption is often linked to work-related stress.
The prevalence of alcohol consumption among adolescents varies from one country to another. In Benin and Cameroon, the prevalence was 30.1% and 87.9% respectively,11,12 while in Tunisia it was 19.6%,13 and in Congo-Brazzaville and Côte d’Ivoire ,5,14 it was 22.8% and 36.1% respectively. These differences can be attributed to the context and the population studied. In this study, the participants were adolescents and young adults aged 15 - 24 living in households, whereas in Burkina Faso, the study focused on secondary school students, which may explain some variations in prevalence. Therefore, it is necessary to take evidence-based measures targeting this age group to reduce alcohol consumption and to recognize the role of the family and community in preventing and promoting alcohol consumption. It is necessary to regulate the marketing of alcohol and to guarantee the availability of alcohol addiction treatment services that strengthen the confidence of young people. Civil authorities will need to ensure that anti-alcohol laws are strengthened, particularly regarding the age of the person authorized to access establishments serving drinks and the age of eligibility for the purchase of alcoholic beverages.
The average age of first alcohol consumption was 7.4 ± 2.7 years, which explains why most of our respondents had their first experience with alcohol in childhood. This very low average age could be explained by the fact that in the city, some parents allow their children to taste alcohol despite their age, at events, ceremonies, and parties, especially in the suburbs. These results differ from those reported in Côte d’Ivoire (10-14 years for girls and 15-19 years for boys). The age at the first alcohol consumption varies by country, with average ages of 16 years in Kinshasa in 2010 and 17.6 ± 2.8 years in Tunisia.7,15 Because the age in this study remains alarming, hence the recognition of the role of the family and communication on the harmful effects of early alcohol consumption in children.
This study showed that 30.9% of respondents who had consumed alcohol reported beer as their first drink. These results are consistent with studies conducted in Côte d’Ivoire and Kinshasa.7,14 The availability and accessibility of beer are a significant factor influencing alcohol consumption among adolescents and young adults.5
Most adolescents and young adults (65.2%) reported consuming alcohol in a bar or on a patio, usually with friends or peers. Regarding motivation, 38% of participants drank to quench their thirst or to imitate others. Similar reasons were reported by Kayembe, who found that thirst, the desire to drink, and the need to imitate peers motivated alcohol consumption among adolescents and young adults.7 Similar results have been reported in Canada, where adolescents consumed alcohol either out of desire or by imitating their peers.16 This sufficiently proves the influence of peers on alcohol consumption and implies severe measures from the various parties and especially the family regarding the education of children.
There was a significant influence between having an income-generating activity, regardless of the type of activity, and alcohol consumption adjusted OR=3.26 (2.04 to5.2), with a p-value <0.001. Adolescents and young adults with an income-generating activity were more likely to consume alcohol than those without. These results are consistent with those of Kayembe, who identified income-generating activities as a determinant of alcohol consumption among adolescents and young adults.7
Limites
The cross-sectional study did not allow for a precise determination of the cause-and-effect relationship between alcohol consumption among adolescents and young adults and the identified determinants. Therefore, the deliberate nature of the respondents’ self-reporting may have introduced a recall bias “information bias”.
CONCLUSIONS
Alcohol consumption is a major public health issue due to its contribution to morbidity and mortality. While prevention policies target the general population, adolescents and young adults constitute a critical group for intervention. Implementing a participatory community approach that engages both individual and institutional levels can improve the effectiveness of prevention efforts within this age group, but political authorities must also be vigilant regarding the marketing of alcohol to this population.
Acknowledgements
To the adolescents and young adults for willingly participating in this study and to the co-author for their commendable contributions and support throughout the process.
Ethics statement
The study protocol was approved by the Ethics Committee of the Kinshasa School of Public Health (approval number: ESP/CE/119/2024). The study adhered to fundamental ethical principles. Participation was voluntary, and confidentiality and anonymity were guaranteed. Written informed consent was obtained from each participant before data collection. For participants under 18 years of age, parental or guardian consent was also obtained.
Funding
This study did not receive any external funding
Authorship contributions
Fidelie LOMBE Bukole designed the study, collected the data, performed the analyses, and wrote the original version of the manuscript. Godefroid MUSEMA MULAKILWA supervised and facilitated the entire process. He reviewed the various preliminary versions and guided the writing of the manuscripts. Corneille Muamba participated in the development of the ODK data collection tool. Christian Lombe participated in the collection of data from adolescents. All authors read and approved the final version of the manuscript.
Disclosure of interest
The authors completed the ICMJE Disclosure of Interest Form (available upon request from the corresponding author) and disclose no relevant interests. The authors declare non-competing interests.