Universal Health Coverage (UHC) is a global initiative for achieving the fundamental right to health.1 It is embedded in the Sustainable Development Goals (SDGs) by the United Nations (UN).2 Besides improving health, UHC is meant to enhance financial well-being, equity, and economic development.3 All UN members have set a 2030 timeline for the achievement of UHC as part of SDGs.4 Many countries globally have focused on reforming national policies to accommodate the UHC agenda.3 The Political Declaration of the UN high-level Meeting on UHC reaffirmed the ambition to achieve UHC.5 The progress toward UHC is likely to be fast if countries take charge of improving access, affordability, and quality of care. Enhancing everyone’s access to quality healthcare services without increasing the risk of financial hardship is the pathway to UHC.6 Individual countries can best achieve UHC by addressing factors unique to them since there is no a one-size-fits-all strategy.7 Applying varying strategies implies that countries are likely to achieve UHC implementation at different times.
African countries have huge disparities in UHC activities. Eleven African countries were in the lowest decile in the ranking of world countries on UHC effective coverage indices,8,9 possibly due to low rates of UHC policies and activities. Interpreting findings of systematic reviews on UHC activities in Africa without considering the patterns of publication activities is likely to misconstrue the performance of countries with the most publication activities as representative of continental performance.10 Therefore, a study that shows variations in UHC publication activities across Africa is needed for contextualization of evidence in systematic reviews toward identification of the interventions needed for UHC progress in various parts of Africa.
A systematic mapping study organizing publications on UHC by African sub-regions where the studies were published can reveal the geographical patterns of scholarly activities regarding the various aspects of UHC. Researchers can then leverage the systematic maps to determine the evidence-generation activities they should initiate in the various African regions to fill literature gaps. The systematic maps can also simplify the identification of role model African countries where effective implementation of various aspects of UHC can be learned. The aim of this systematic mapping study is to describe the patterns of UHC-related publication activities across African countries as revealed by publication patterns. It will improve the understanding of UHC implementation across Africa and guide African researchers and policymakers in identifying UHC aspects that ought to be prioritized in different countries.
METHODS
Research method
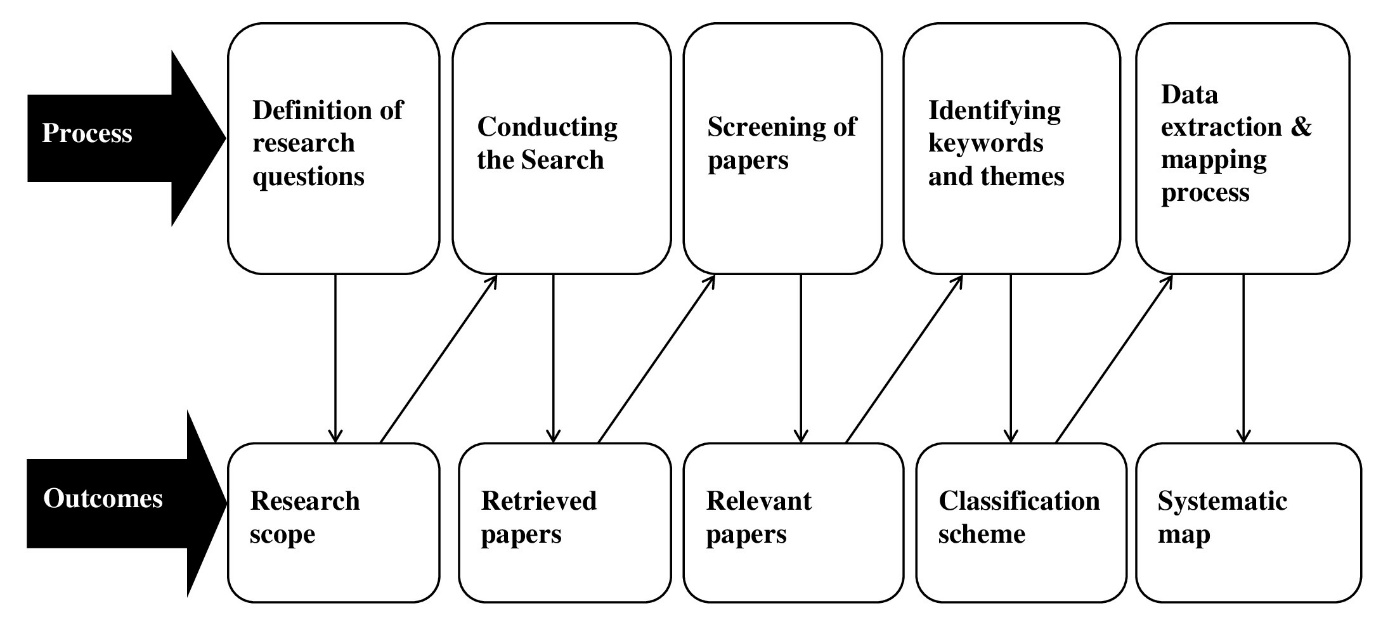
This systematic mapping study was conducted following the mapping process (figure 1) described by Petersen et al.11 and Petersen et al.12 and applied in health research by Ngayua et al.13 The mapping process started by outlining the research questions, listing the relevant search terms, and searching for publications addressing the research questions. Document selection was based on predefined inclusion and exclusion criteria. Keywords specific for the research questions were identified upon which a scheme was developed for classifying them, extracting data from publications, and mapping the data accordingly.

Definition of research questions
This systematic mapping study aimed to contribute to the documentation of the WHO African region (WHO AFRO) transformation agenda by describing UHC-related publication patterns. The WHO AFRO secretariat and other stakeholders will leverage the findings of this study to provide the best possible technical support for UHC evidence generation to countries in Africa as per WHO’s vision for UHC in Africa outlined in the Africa Health Transformation Programme.14,15 The main research question addressed in this systematic mapping study is:
What is the status of evidence regarding the implementation of UHC across Africa?
Three study objectives were set to facilitate addressing the research question. They include:
-
To describe UHC-related publication patterns in Africa based on type of publication, location of published activities, contribution to UHC, and aspect of UHC addressed.
-
To identify current trends in the publication of UHC implementation and examine the value of the publications in fast tracking the implementation of UHC across Africa.
-
To pinpoint information gaps that researchers and organizations can fill through targeted research and documentation activities.
Six research questions were then derived from the three objectives. They were composed to induce synthesis of information regarding publication of UHC activities in Africa. The research questions (RQs) include:
RQ1: Which types of publications have documented the milestones African countries have made in the journey to attain UHC?
Rationale: Analyzing the articles by type is essential to determine the level and quality of evidence on UHC activities in Africa. The type, quality, and evidence level of publications were deduced. Determination of evidence level was based on the study design-based hierarchy of evidence. For example, a research article published upon a cohort study has a higher level of evidence compared to a research article based on a cross-sectional study.16
RQ2: What are the major contributions of the publications to the issue of UHC implementation in Africa (essential package of health services, health financing approach, and healthcare access barriers)?
Rationale: Answering the question revealed the value of the publications in advancing the implementation of UHC through the three pillars of UHC including quality, affordability, and accessibility of healthcare services. The advancement is attained through the provision of an essential package of healthcare services, streamlining health financing, and addressing access barriers.17 Disparities in the extents of publications’ contributions into each of the three UHC pillars were leveraged to depict the UHC pillars that have been scantly addressed.
RQ3: Which aspects of UHC have the retrieved publications addressed (improvement of primary health care, change of health outcomes, performance of health systems, and addressing of health determinants)?
Rationale: Obtaining evidence to answer the question showed the variations in the extents to which the various aspects of UHC have been addressed in the publications. Aspects of UHC that have been extensively studied were described while aspects that needed more publication activities were identified.
RQ4: Which programs have stakeholders implemented towards UHC in Africa (advocacy, UHC index surveys, strategic planning, policy-making, resource mobilization and resource supplementation, and measurement of progress)?
Rationale: Analyzing the programs that various stakeholders have implemented to support UHC implementation unearthed areas that need heightened activity. It showed programs that have been extensively replicated. Stakeholders can leverage the information to avoid further proliferation of extensively replicated interventions and intensify neglected UHC activities.
RQ5: How has the publication of information on UHC in Africa evolved over the years?
Rationale: Analyzing changes in the UHC activities as reflected by publication activities over the years was essential to determine whether the transformation over the years is toward the right direction. Emerging, neglected, reemerging, and relevant themes were identified, thus providing background information on the approaches to shape the implementation of UHC in the future.
RQ6: How does the frequency of UHC-centered publications in Africa vary by country and sub-African region?
Rationale: Comparing the frequency of publications across countries and sub-African regions showed areas where UHC implementation is progressing fast or derailing. Countries that are in the early stages of UHC implementation can identify mentors from among nations with relatively high UHC-related publication rates, as stakeholders identify countries that need the most urgent UHC-related support.
Conducting the search
Search terms to facilitate the identification of relevant publications that would answer the research questions were developed. The search engines where the publications were searched were specified.
Search criteria
Only phenomenon and context were relevant in the definition of the searched terms. The phenomenon of interest was universal health coverage. The context was the African region. Thus, the keywords searched include: “universal health coverage” OR “UHC” OR “universal healthcare” OR “health financing” OR “health insurance” AND “Africa” OR “African region.”
Data sources and search process
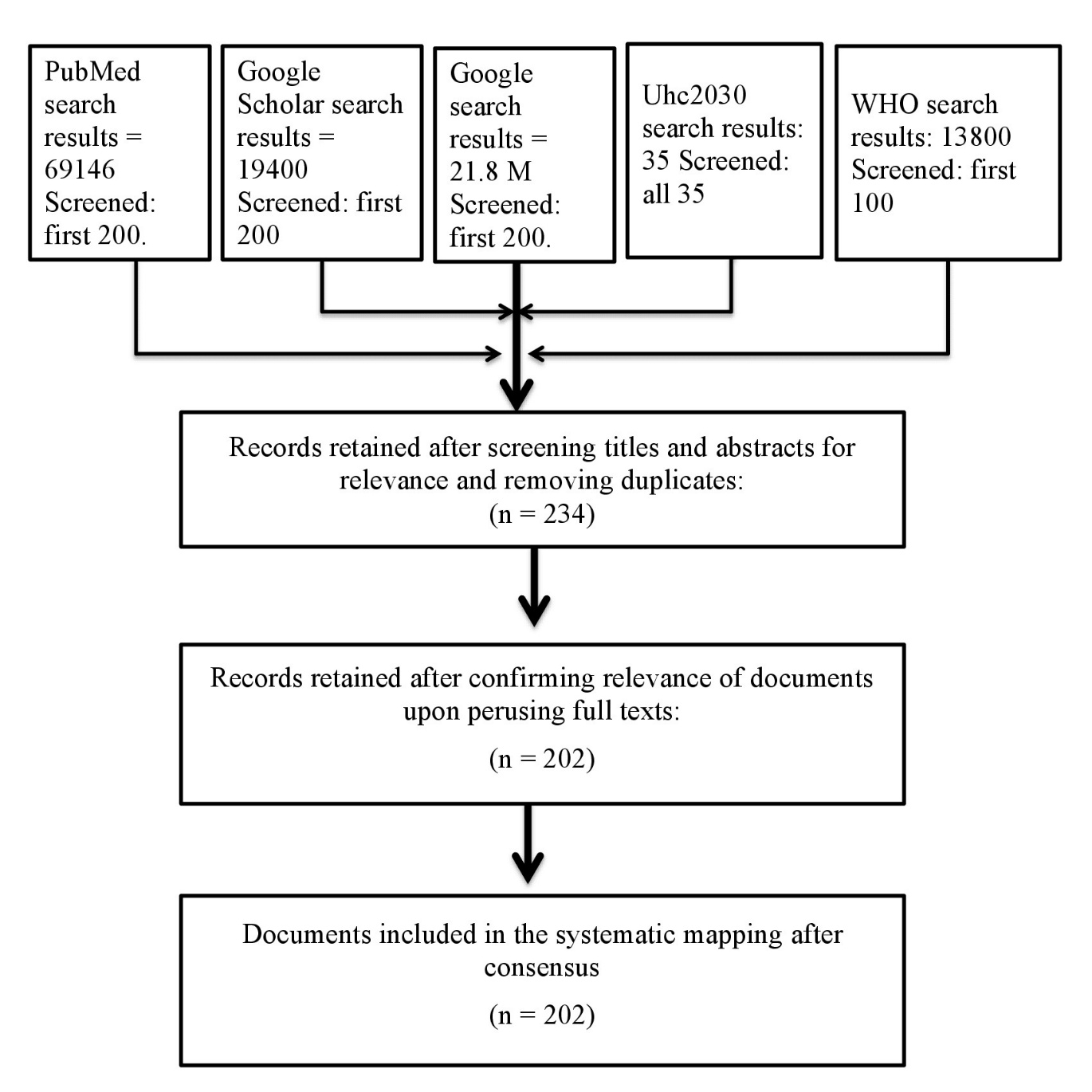
The search engines used to identify the relevant publications include the WHO AFRO publications, uhc2030, PubMed, Google Scholar, and Google. Combinations of the key terms were searched from 1stApril 2023 to 30th April 2023. Only documents published between 2013 and 2023 were included since the United Nations General Assembly initiated acceleration towards achieving UHC globally by endorsing a resolution on Global Health and Foreign Policy on 12th December 2012.18 Only documents published in English were selected. The keywords searched in each engine and the number of results obtained are shown in table 1.
Screening of papers
Filters were applied in the search engines to limit the articles included in the systematic mapping study to articles published between 2013 and 2023. The search results were perused to identify titles on UHC in Africa. The abstracts, summaries, or executive summaries of relevant titles were read to ascertain the relevance of the documents. Full-text was read if the relevance of a publication was not apparent after reading the summary.
The inclusion criteria were documents:
-
Directly addressing UHC in Africa authored inside and outside Africa
-
Published between 2013 and 2023.
-
Published in a peer-review journal or by an authoritative organization.
-
Available in English.
-
Accessible in full-text.
The exclusion criteria were documents:
-
Published as preprints.
-
About non-African populations in Africa
-
Authored or sponsored by for-profit organizations.
-
Marketing products.
-
Published as news articles, speeches, or remarks
The screening of the documents to identify the ones that met the inclusion and exclusion criteria was done by the primary author and ascertained by the secondary authors. A flow diagram (figure 2) adapted from the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) was followed when selecting articles.19

Identifying keywords and themes
Keywords from the articles were leveraged to develop themes that would facilitate the answering of the six research questions. Two classification schemes, the fixed and topic-specific classification schemes, were selected for grouping the articles. Then, six facets were designed based on the relevance of the document details and themes to the six research questions. Publication year, publication type, publication location, and contribution facets were designed within the fixed classification scheme. On the other hand, publication focus and publication dimension facets were designed within the topic-specific classification scheme. The selected documents were placed in the classification schemes and the six facets.
The publication year facet facilitated the development of a systematic map displaying the annual frequency of publications. The publication type facet (table 2) enabled the mapping of the nature of the progress in UHC.
The location of publication facet was based on the sub-African region where the activities leading to the publication were conducted. The primary author categorized countries into commonly known regions including Southern Africa, East Africa, Equatorial Africa, West Africa, and North Africa (table 3).
The contribution facet was based on the information that the various publications provided toward understanding the progress African countries have made in the implementation of UHC. The categorization of publications based on their contributions resulted in three contribution facets including package, financing, and access consistent with the three UHC pillars (table 4).
The publication focus facet was based on the aspect of UHC addressed. Four facets were developed based on the foci of the documents: primary healthcare, change of health outcomes, performance of health systems, and addressing determinants of health (table 5).
The publication dimension facet was about the aspect of the UHC implementation pipeline that the document was addressing. Several programs contribute to the implementation of UHC; they are initiated based on the stage of the UHC implementation process. They include advocacy, policy-making, strategic planning, resource mobilization and supplementing resources, index surveys, and progress assessment (table 6).
Data extraction and mapping process
Each article was read to extract data regarding the six facets. The data were entered into an excel sheet as per the classifications scheme. Data analysis started by obtaining the frequency of publications in each category, which were utilized to develop the systematic maps. Bubble plots facilitated the establishment of the systematic maps for the various facets. Scatterplots (x-y) were created such that bubbles of different diameters depicted the number of publications with the intersecting features. Thus, the diameters of the bubbles corresponded to the frequency of publications that fit the criteria of the intersecting facets.
Data synthesis answered the research questions on the progress the African continent has made in the publication of UHC activities in Africa. The observer triangulation method was applied to ensure rigor in the classification of the articles and the development of systematic maps. The developed systematic maps show the distribution of UHC-related documents published between 2013 and 2023 in Africa.
RESULTS
Mapping results
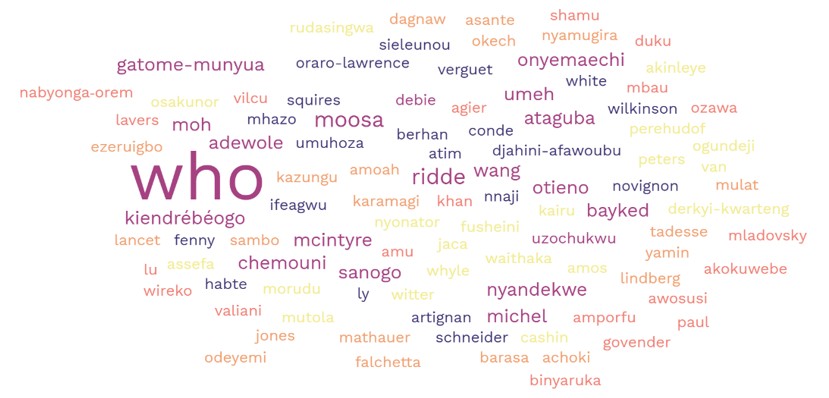
The identification of technical publications on universal health coverage in Africa from among the first 200 search results in each of the five search engines yielded 202 relevant publications. WHO was the main author of the publications by authoring 17 documents; Moosa and Ridde were the other major primary authors with three publications each (figure 3).

Publication types (RQ1)
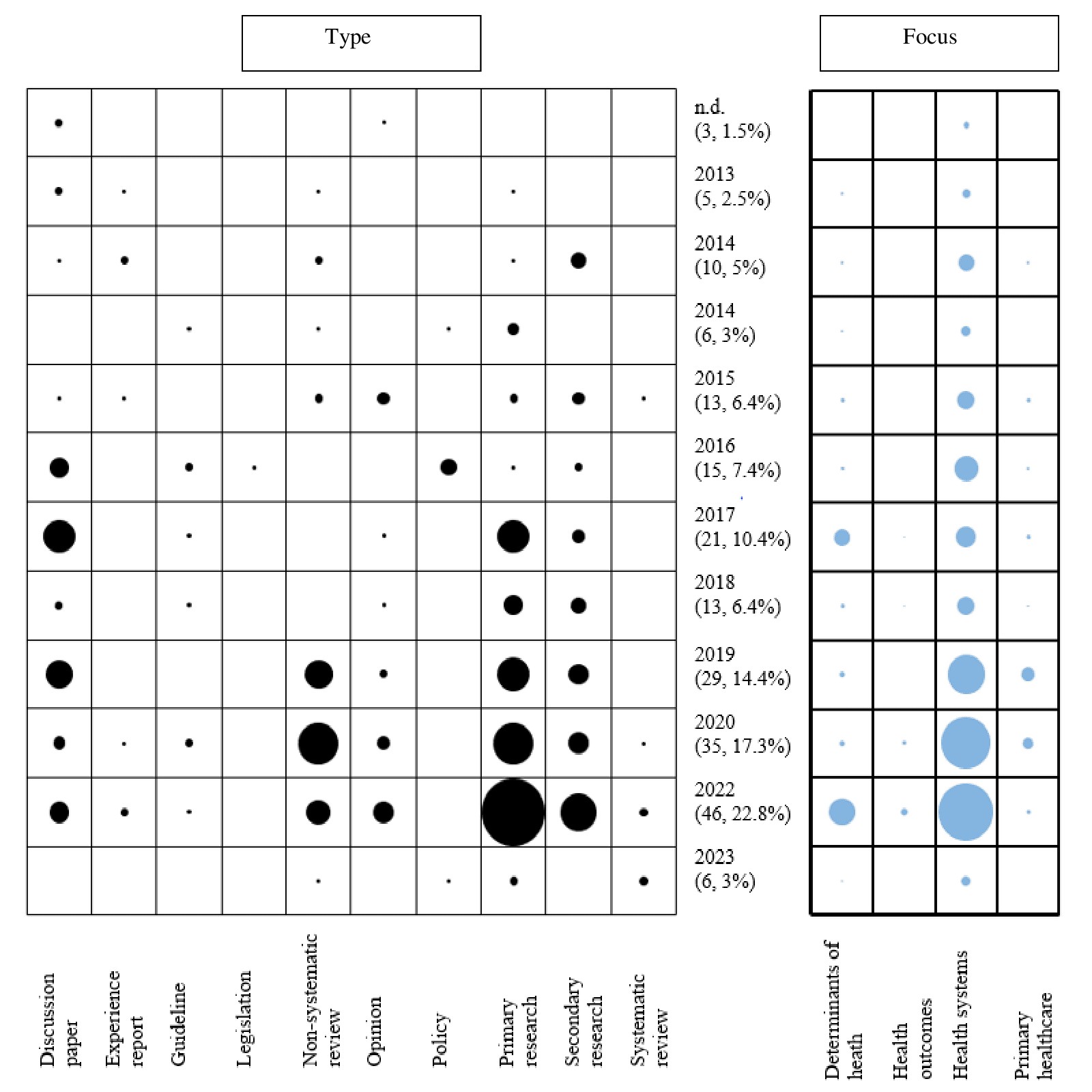
Majority of the publications were primary research papers (28.2%, n = 57), discussion papers (17.8%, n = 36), and secondary research papers (17.3%, n = 35) (figure 4) (table 7). The primary research studies applied a qualitative research approach comprising document review and interviews to collect data on UHC activities. Secondary research articles had results of analyzing data collected in previous UHC-based research activities and implementation processes.

Only a single legislation (0.5%) was retrieved from the search process. Other scanty types of publications include policies (3.0%, n = 6), systematic reviews (3.0%, n = 6), and experience reports (3.5%, n = 7). Legislation and policies were mostly government documents regarding the commitment to implement UHC. Experience reports were mainly descriptions of encounters in the process of implementing the UHC activities.
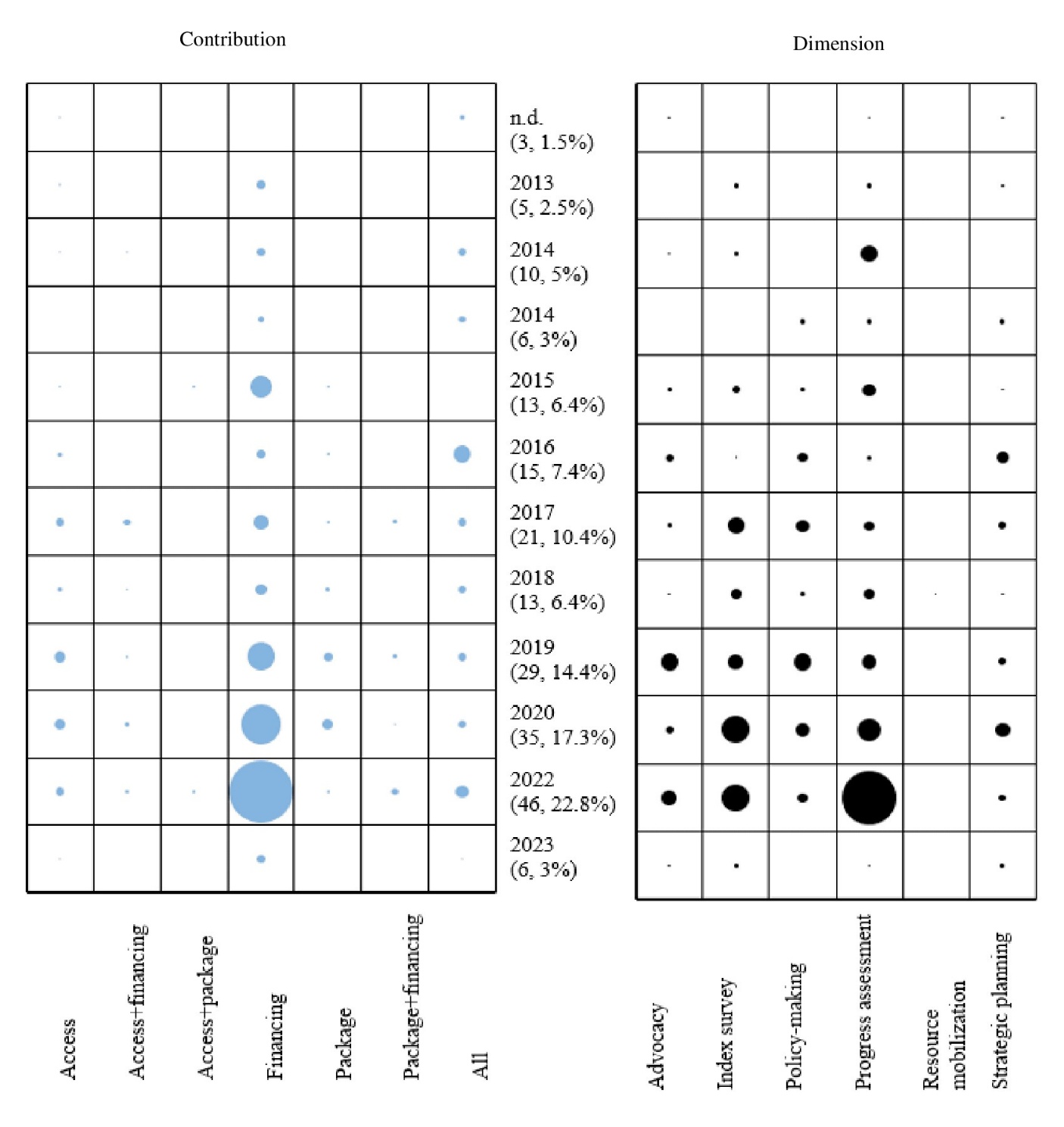
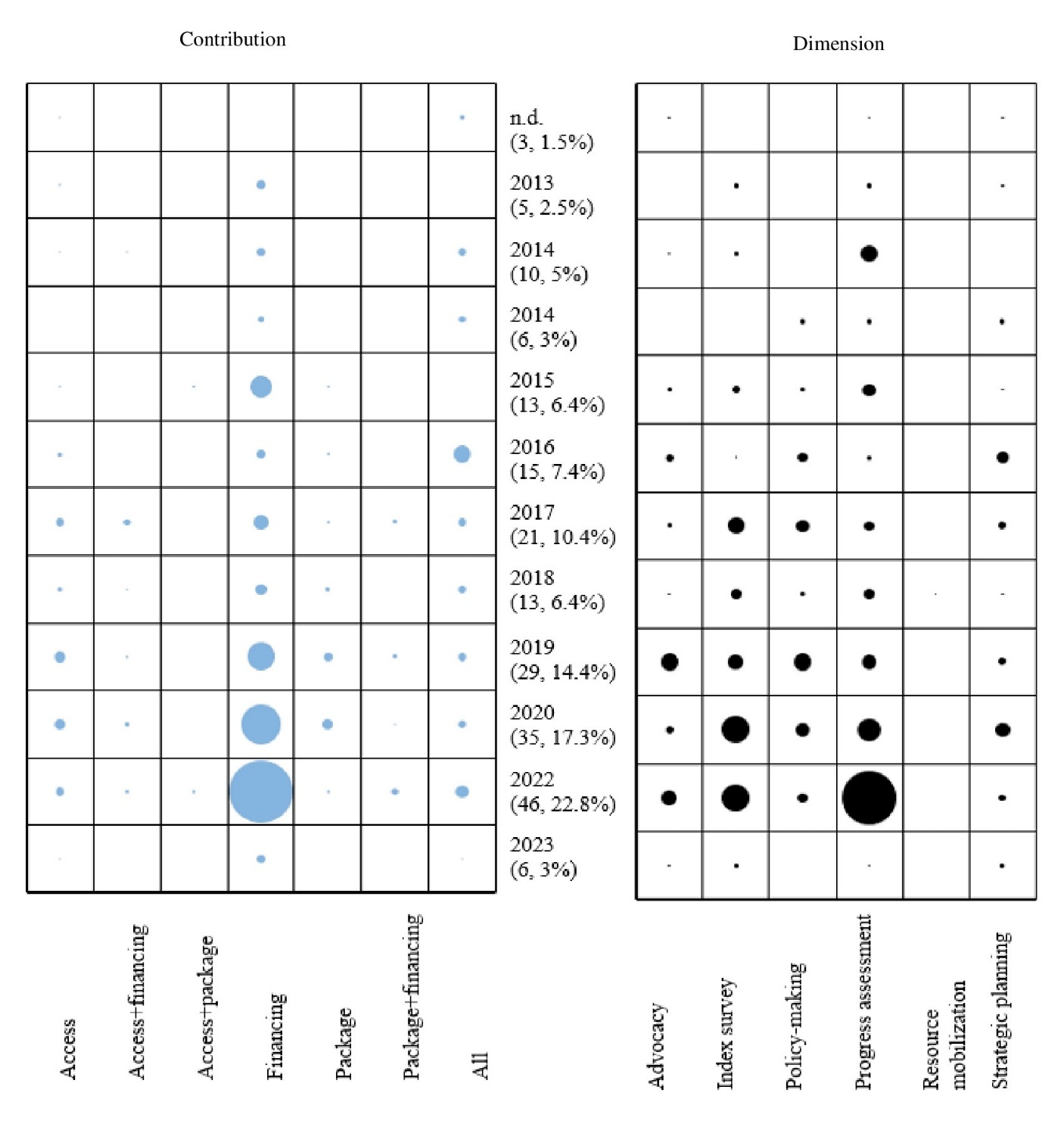
Contributions (RQ2)
The contributions were categorized as per the three pillars of UHC including package, financing, and access (figure 5). Half of the publications (n = 101) were about the financing of UHC (table 8). The publications on financing were mainly primary research articles (n = 31), non-systematic reviews (n = 20), and discussion papers (n = 16). They mainly addressed health insurance, health financing approaches, UHC financing models, and challenges and solutions in UHC financing.
The contribution category second to the financing category comprised articles addressing all the three UHC pillars including package, financing, and access (19.3%, n = 39). Almost half of them comprised discussion papers (n = 12) and guidelines (n =6). Most of the papers discussed milestones countries have made toward UHC, the effects of certain interventions on the UHC journey, and analysis of concepts related to UHC.
Only 7.4% (n = 15) publications specifically addressed the package of UHC services covered by the health insurance programs of countries. They were mainly primary research articles (n = 4) and secondary research articles (n = 4). They contributed information about various components of the UHC package including facilities, healthcare technologies, essential medicines, public health, and research.
The access pillar was specifically addressed in 13.4% (n = 27) publications (table 8). Most were primary (n = 9) and secondary (n = 7) research articles. They addressed the distribution of healthcare facilities, inequities in access to healthcare, and workforce densities. Only a single experience report and a single policy document addressed the access pillar of UHC.
Study focus (RQ3)
More than two-thirds of the retrieved publications focused on performance of health systems (figure 4). Primary research articles (n = 35), discussion papers (n = 30), and non-systematic reviews (n = 21) were the commonest publication types with the performance of health systems focus (table 9). The captured items of health systems include health system functionality, health financing reforms, global health agenda, levels of health insurance coverage, logic models for UHC solutions, and the effect of interventions, among others. Only one legislation, four systematic reviews, and five policy papers addressed performance of health systems.
Publication dimension (RQ4)
Out of the six dimensions, progress assessment was the most predominant while resource mobilization was the least (figure 5 and table 10). Examples of progress assessments captured in the publications include analyzing levels of health insurance coverage, assessing benefits and challenges of UHC, and measuring health service utilization.
Publication Years (RQ5)
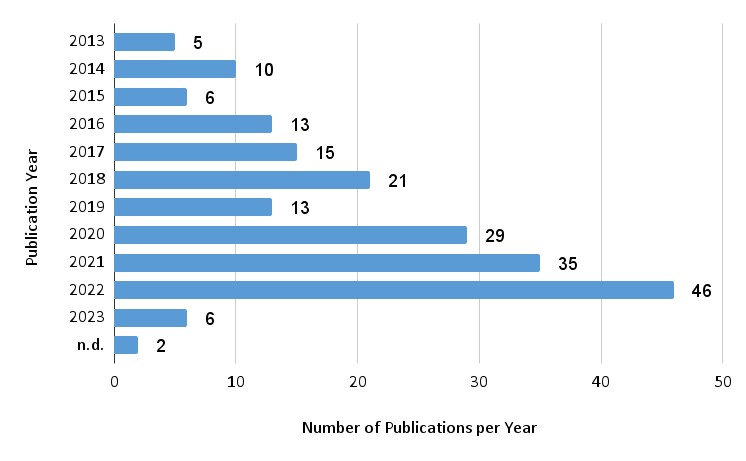
The number of publications about UHC in Africa appearing among the first 200 search results steadily increased from five in 2013 to 46 in 2020. Fifty-five percent (n = 110) of the documents were published between 2020 and 2022 (figure 6).

The publication of primary and secondary research articles progressively increased over the years. Between 2013 and 2017, primary research articles ranged from one to three. Between 2018 and 2022, they increased to between five and sixteen articles. Similarly, secondary research publications increased from two to four between 2013 and 2020 (table 11).
Frequency of publications by countries and sub-regions in Africa (RQ6)
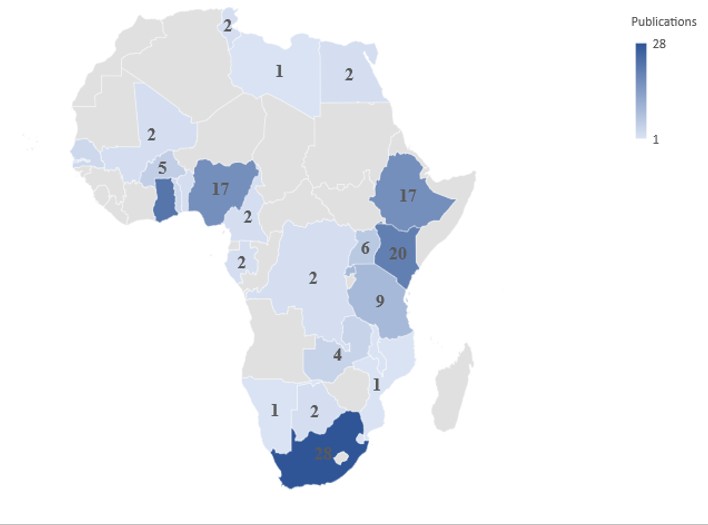
The publication activities on UHC were concentrated in a few countries since only 18 countries had some publications. The publications seem to be concentrated in countries in East, West, and South Africa (figure 7).
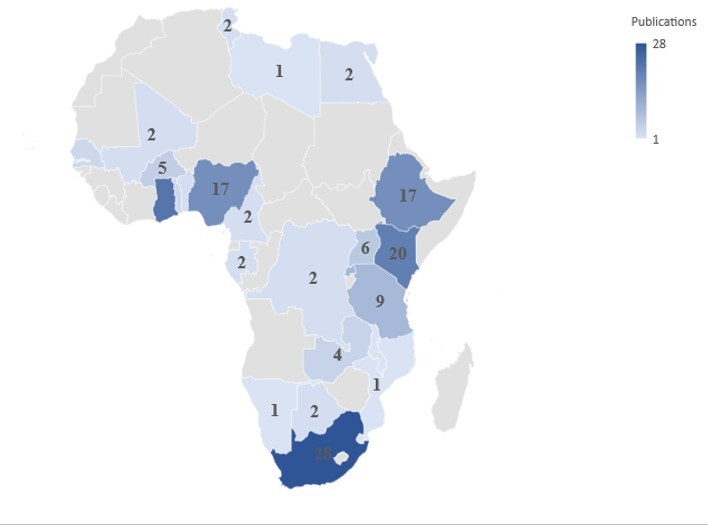
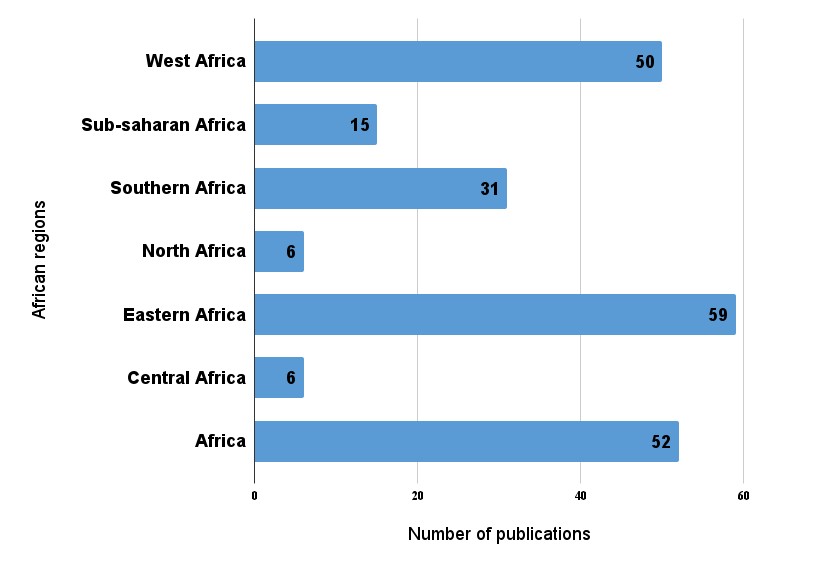
East Africa had the most publication activities followed by West Africa (figure 8). North Africa and Central Africa had the least UHC-related publication activities. Some articles covered Africa as a whole while others covered Sub-Saharan Africa as a single region.

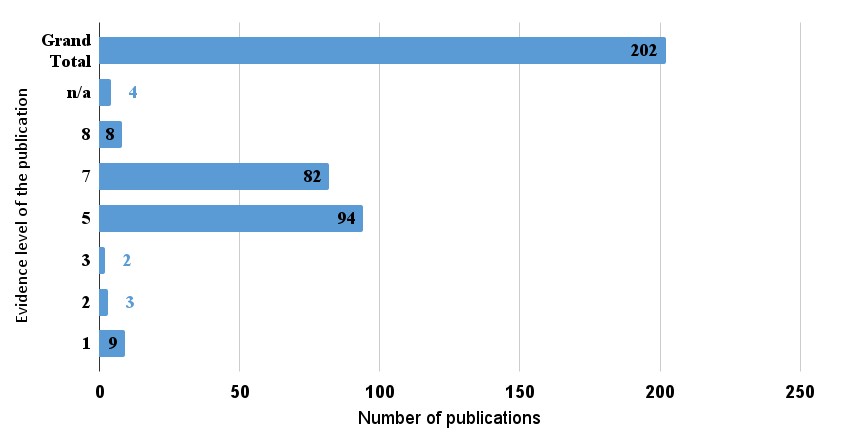
Level of evidence and quality
Most publications had level 5 or 7 evidence. High-level evidence research articles such as systematic reviews, clinical trials, and cohort studies were scanty (figure 9).

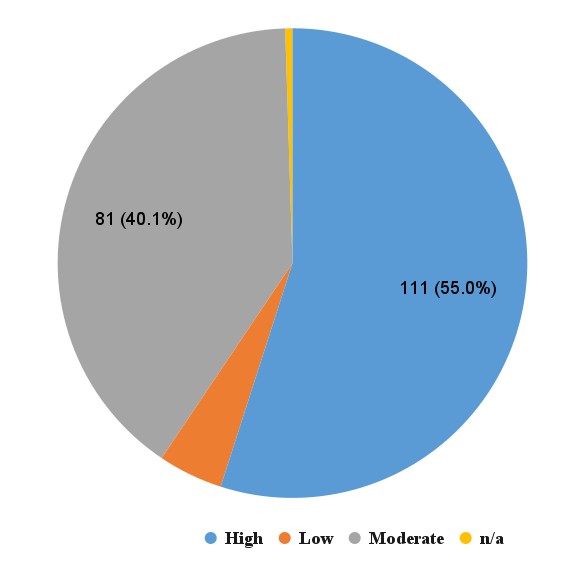
Subjective assessment of quality of the publications based on quickly checking comprehensiveness, fidelity to study design, and clarity of communication of findings revealed that most of the publications were of moderate or high quality (figure 10).

DISCUSSION
Evolution of publications (number and type)
The steady increase in publication of technical documents regarding UHC between 2013 and 2022 could be due to rare and unclear application of implementation research to support UHC activities in Africa in the past, hence the scarcity of related publications in the early years.27 The trend of increasing quantity and quality of publications could be due to researchers and implementers producing more UHC information from their activities as time progresses. Monitoring and learning systems implemented alongside UHC may be contributing to the increasing UHC publications in the implementation processes.28
Most African countries could be in the formative stages of implementing UHC considering the scarcity of high evidence-level materials. Thus, countries are yet to substantially integrate UHC into healthcare systems for availability of data to substantially evaluate UHC’s impact and document implementation experiences.29 Retrieval of experience reports for South Africa, Ethiopia, Tanzania, and Rwanda – countries that also had high numbers of other types of UHC-related publications – implies they may have made notable milestones in the overall implementation process.
Since legislation and policies are the transition points from research activities into implementation, their scarcity amongst the first 200 search results implies that most African countries are yet to reliably commit to UHC implementation.30 Nevertheless, the proliferation of initial research steps as evidenced by the numerous primary and secondary research papers implies establishment of a concrete foundation for the UHC process.
Contributions of publications to UHC implementation
The identified publications were about activities to support the implementation of UHC. The factors explored in the publications including political will, inequities, health financing mechanisms, human resources, and countries’ commitment to the UHC journey point to the facilitators and barriers to UHC implementation.27 Implementation gaps such as the scarcity of evaluation and experience reports can be leveraged to initiative research, development, and evaluation activities to make UHC implementation comprehensive.
The identification of financing as the commonest contribution facet is consistent with the fact that affordability of healthcare is the greatest challenge in the implementation of UHC.29 African countries have challenges financing their healthcare systems, hence it is promising to observe that authors in the continent are striving to find solutions to the financing challenges.30 The overdependence on out-of-pocket spending on healthcare, which is prevalent in Africa, is not consistent with the core tenets of UHC.31 Hence, the efforts by African countries to establish health insurance schemes is commendable.
Aspects of UHC addressed by the publications
Most UHC activities were about improving health systems and addressing determinants of health. According to Sturmberg and Martin,31 developing a system-wide framework to transform healthcare is the basis of achieving UHC. Only a few publications addressed primary healthcare and health outcomes. Yet, WHO considers transforming primary healthcare as the quickest way to achieve UHC.32 African countries should position primary healthcare as the cornerstone of the strong health systems they seek to establish for UHC.
The focus on social determinants of health (SDH) at the foundation of UHC in African countries indicates a potential for healthcare systems that promote equity. Factors such as education levels, housing, income levels, and environmental exposures affect health and cause variations in disease burdens across populations, thus entrenching inequities.33 The socioeconomic disparities among populations in African countries makes integrating the addressing of SDH a priority to avoid worsening the inequities. The UHC-geared multisectoral interventions targeting various SDH are likely to improve health outcomes,34 thus achieving the end goal of UHC of better health and attaining SDGs. They are also intent on ensuring equitable access to health by addressing SDH, which is likely to result in better health outcomes.
Pro-UHC programs implemented in Africa
The high number of publications on index surveys and progress assessment show an interest to transition UHC from policies into actual implementation. Index surveys lay ground for the initiation of UHC activities while progress assessments indicate the milestones that countries have made in the UHC journey. Availability of data, which is facilitated by the index surveys and progress assessments, is critical in identifying challenges and opportunities that can be addressed to improve performance.27
The balancing of advocacy, policy-making and strategic planning as evidenced by nearly equal proportions of number of publications shows a multi-pronged approach to mainstreaming UHC in existing healthcare systems. The WHO argues for UHC by supporting advocacy efforts that translate into strategic initiatives embedded in policies for sustainable transformation.6 The policy-making and strategic planning functions of the health systems governance ensure that UHC-related advocacy efforts translate into real progress in UHC.35
WHO contributions in the evolution of UHC-related publications
As the topmost author, WHO contributed policy documents, some that provided the vision for UHC in the African region.15 Other documents discussed how to achieve quality UHC. For example, WHO36 discussed how improvements in water, sanitation, and hygiene services in healthcare settings can be leveraged to achieve quality UHC based on lessons from Ethiopia, Ghana, and Rwanda.
The WHO Regional Office for Africa discussed frameworks for improving specific aspects of UHC and shared experiences on the implementation of UHC in the WHO AFRO. For instance, the document “tracking universal health coverage in the WHO AFRO, 2022” shared the orientations, trends, activities, and strategic shifts across the access, affordability, and quality pillars of UHC.37 Therefore, WHO is integral in the UHC journey in Africa.
Limitations of the study
The search process was not exhaustive due to limiting the search to the first 200 results and excluding some subscription-access publications, which may have left out some relevant publications. However, the restriction was necessary to broaden the search to five databases within the available time and resources. The limitation may not have affected the findings significantly since most readers of publications barely go beyond the fifth page of the search results yet the 200 results occupied 10 pages. Secondly, a risk of possible selection and misclassification bias existed since publication identification and classification were subjective based on the researchers’ understanding of research methods and technical communication and the protocol was not registered. However, the counterchecking of the selected and classified articles by the second and third authors after the first author completed the process and applying the majority rule in cases of disagreements reduced the risk of bias.
Implications for future research and practice
Researchers can identify evidence gaps for further research by checking the systematic maps and picking areas with the least publication activities as a starting point in helping investors identify neglected aspects, programs, and pillars of UHC. UHC stakeholders should increase their publication activities in contributing toward the package and access UHC pillars to match the effort put in financing. More UHC initiatives should adopt the resource mobilization and strategic planning dimensions since they are the least captured in the mapped publications. Additionally, publications on primary healthcare interventions and measurement of health outcomes should be increased for the UHC journey to be comprehensive. Furthermore, publication of experience reports, legislation, guidelines, and policies should increase for a balanced approach in communicating the UHC efforts in Africa.
The revelation of the scarcity of high-evidence publications challenges researchers, policymakers, and sponsors to transition from conceptualizing, discussing and opinionating on UHC. They should advance into testing interventions, evaluating activities, and systematically reviewing well-designed primary research articles to generate high-level quality research evidence on UHC. The transition will further improve the quality of UHC-related publications generated in the African region.
UHC policymakers and implementers in specific countries should engage WHO Regional Office for Africa in their implementation efforts to leverage its experience supporting UHC initiatives in Africa. They can partner with the WHO Regional Office for Africa to build on the achieved milestones. Further research is recommended to rule out the low likelihood of publishing in English as an explanation for the observed low UHC-related publications rates in North Africa and Central Africa.
CONCLUSION
Africa’s high disease burden, weak healthcare systems, and socioeconomic challenges necessitate fast tracking of the UHC implementation processes. Governments and international partners led by WHO conduct UHC-related activities in Africa often communicated through publications. This systematic map shows that UHC-related publication activities and quality progressively increased between 2013 and 2023, although mainly in about a third of African countries. WHO was at the center of the UHC-related publication activities, which mainly revolved around health systems financing and performance. UHC implementation stakeholders and researchers can leverage the systematic maps to identify areas such as legislation and evaluation of UHC implementation to spur activities and publications for equity in UHC progress and communication across Africa.
Data availability
All data generated or analyzed during this study are publicly accessible through: DOI: 10.17632/gxmx968mwh.1
Competing interests
DK is an independent consultant contracted by WHO Regional Office for Africa to conduct this systematic mapping study. AMA and KN are WHO Regional Office for Africa’s staff members.
Funding
This systematic mapping study was funded by WHO Regional Office for Africa.
Author’s contributions
DK proposed the study, conducted the search, systematically mapped the publications, and wrote the initial draft of the manuscript. AMA verified the relevance of the selected studies and the accuracy of the systematic mapping process, and proofread the manuscript. KN verified the classification, proofread the manuscript, critically appraised the content, and suggested areas of improvement. All authors read and approved the final manuscript.
Disclosure of interest
The authors completed the ICMJE Disclosure of Interest Form and disclose no relevant interests.
Correspondence to:
Dennis Kithinji
Medright Consulting LTD
P.O. Box 313-60600
Kenya
dennohkithinji@gmail.com
Kizito Nsarhaza
WHO AFRO
P.O.Box 06 Brazzaville
Republic of Congo
nsarhazak@who.int