INTRODUCTION
Splinting is a technique to stabilize musculoskeletal (MSK) injuries such as fractures and dislocations, serving as a first-line treatment to limit movement, protect tissues, and reduce pain during healing.1
Treatment of musculoskeletal injuries is a high priority worldwide, as indicated by the Global Burden of Disease data that found 1.71 billion people live with MSK injuries leading to chronic disability.2 This data, however, does not reflect the difference in MSK prevalence between high income countries (HIC) and low-to-middle income countries (LMICs). MSK injury burden in LMICs is a significant problem due to limited healthcare resources, such as infrastructure, supplies, human resources, and formal education for treating such injuries. Lack of resources often lead to increased undesired outcomes and neglected conditions.3,4
An example of such undesired outcomes can be seen in Nigeria, a LMIC where Traditional Bone Setters (TBS) commonly treat MSK injuries. TBS are apprenticed bone healers who typically received ancestral information without formal scientific training.5 TBS treatment accounts for 70-90% of the primary fracture care in parts of Nigeria yet have a high reported complication rate of 66.7-83%5 including joint stiffness, malunion and nonunion of fractures, compartment syndrome, systemic infection, toxemia, limb gangrene and death.6 The limited number of orthopaedic surgeons in Nigeria,7 coupled with the frequent complications associated with TBS care suggest that access to basic MSK treatment skills and materials for splinting could potentially alleviate the high demand for MSK care in Nigeria and countries alike.
Successful splint properties include bone immobilization, moldability, ease of application, availability, and cost. First, for a splint to provide immobilization for bone repair, it must contain intrinsic strength that can hold a limb or joint in the desired position.8 Second, to create a patient-specific immobilization device, the splint material must be easily moldable.1 Third, splinting should be an easy application process for healthcare professionals. Lastly, splinting materials must be readily available, either purchased at an affordable cost, or easily manufactured. If a splint possesses these properties, trained healthcare workers should be able to immobilize a limb with decreased rates of complications such as nonunion, limb gangrene, and infection.
Although plaster and fiberglass are readily available and suitable for modern orthopedic care,9 no study has evaluated the practicality of these splints in LMICs for resource allocation. This review aims to provide an overview of current orthopedic splinting materials and perform a qualitative cost-benefit analysis of these materials to understand the feasibility and potential effectiveness in the context of LMIC use.
METHODS
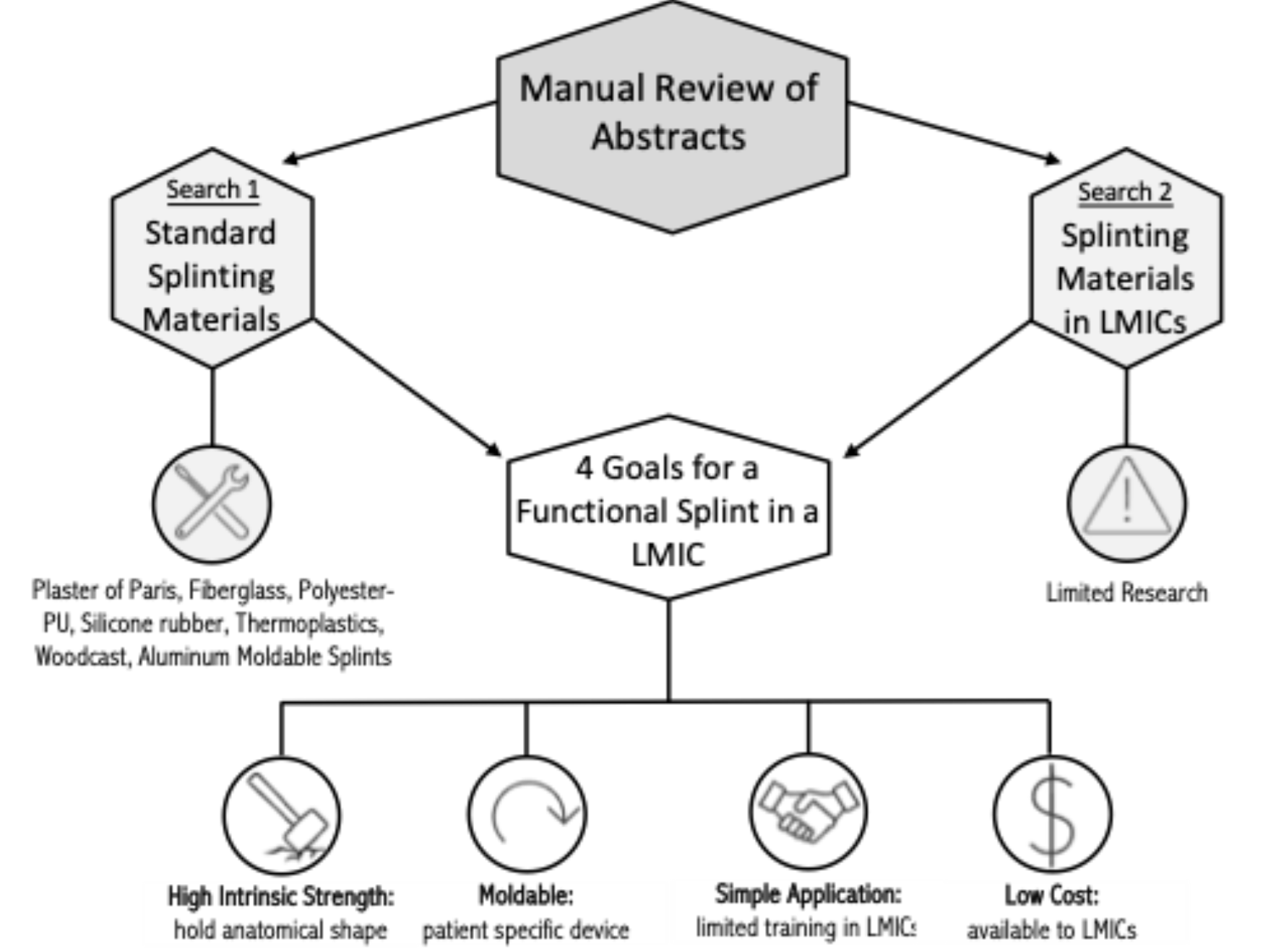
A literature review was performed using PubMed, Web of Science, and Google Scholar databases over the past 10 years to identify the current standard splinting materials available. This search included keywords such as splint, splint materials, splinting principles, alternative splint materials and splint costs. All literature discussing splinting materials for MSK injuries were included while orthodontic splinting was excluded for a total of 13 papers reviewed. The most common materials identified were plaster, silicone rubber, fiberglass, polyester-PU resin, thermoplastics, and Woodcast, consistent with previous literature.9
An additional search into the standard splinting materials mentioned above in low to middle income countries was also performed using databases above, yielding no significant literature. Thus, highlighting the need for further analysis and an area of huge potential improvement with relatively low monetary expense.
Based on our original search, we identified four common qualities that splinting materials share. These include: 1) high level of intrinsic strength, 2) malleability, 3) ease of application and 4) monetary cost. Figure 1 demonstrates a schematic of these methods. A cost-benefit analysis, using these common qualities as distinct goals for a successful splint, for use in LMICs was performed on the seven splinting materials identified above. The cost-benefit analysis used literature from both our searches to provide a qualitative assessment.

Properties of Modern Splinting Materials
Plaster, a gypsum or calcium sulfate hydrate, undergoes an exothermic reaction allowing the crystallization and interlocking of gypsum particles.9 Cotton bandages are impregnated with plaster with additional binders to allow for a stronger gypsum adhesion.9 Different additives can be included to alter the physical properties of the plaster including setting time, bandage adhesion, and moisture.
Fiberglass is activated polyurethane resin impregnated in stretch-relaxed tape.9 It is a lighter weight splint due to number of layers and material composition.9 Fiberglass must be handled with gloves due to skin toxicity, and the short setting time means it must be molded quickly onto the affected limb.9
Polyester-Polyurethane (PU) splints are bandages impregnated with a prepolymer urethane resin.9 It undergoes an exothermic reaction polymerizing into a flexible, crude polyurethane.9 Elasticity, strength and setting time of the splint can be modified by altering the molar ratio of the functional end groups or the molecular weight of the polyol.10 The stabilizers added to the bandage are toxic and challenging to handle. It readily sticks to skin and is attributed with sharp edges that could harm patients if not properly applied.9
Thermoplastic is an impregnated polyester polymer with inorganic fillers on a cotton base.9 Thermoplastic is lighter than and is applied in a similar manner to plaster.9 Low temperature thermoplastic has benefits of being able to be reheated, stretched, remolded and cut with scissors when warm.9 The plastics require high temperatures for activation that can cause thermal damage to patients and lack of elasticity can cause pressure sores.9
Silicone rubber splints were created with the intention of being worn by athletes during play due to its high degree of flexibility.11 Splints can be either reinforced with outside structure such as aluminum, urethane foam padding, or use of medical gauze between layers of silicone.9 Silicone has good force absorption properties and is more effective in short term rather than long term immobilization.9
Woodcast is a biodegradable thermoplastic polymer and woodchip.9 The material is lightweight that is cut to size and molded.9 The wood chips provide insulation limiting the risk of thermal damage to the patient.9 It is non-toxic, self-adhesive and waterproof.9
The aluminum moldable splint is commonly used in the military and wilderness medicine.12 It is composed of two layers of closed-cell foam surrounding a sheet of aluminum on the inside.13
Cost-Benefit Analysis of Splinting Materials in the Context of LMICs
Material strength
Regarding the biomechanical properties of plaster and fiberglass during curing time, a significant difference in the load the splints can withstand was found, with fiberglass having a higher yield and ultimate load than plaster.14,15 Despite plaster being weaker, plaster exhibited less displacement than fiberglass suggesting a stiffer and more brittle material.14 When examining strength and setting time with various NCO/OH molar ratios (functional end groups) and polyol molecular weights of polyester-PU and fiberglass, the polyester-PU splint showed higher compression strength and tensile strength for all end groups and molecular weights.10 Fiberglass was also found to have anisotropic loads, meaning it was stronger across the bandage but not length wise whereas polyester-PU was strong both width and length wise.15 Thermoplastics, although rigid, has been found to have lower weight bearing abilities than fiberglass.9 Compared to fiberglass, Woodcast splints were found to have a lower tensile strength, however, this did not translate to clinical practice as evidenced by no significant difference in splint breakage between wood-composed and fiberglass splints.16,17 The collection of these results demonstrates a strength ranking as: polyester-PU > fiberglass and Woodcast > thermoplastics > plaster. There is currently no literature examining the strength of aluminum moldable splints to allow for comparison and further analysis.
A recent study found no difference in radiographic reduction after 2 weeks using a plaster versus fiberglass splint in pediatric patients.18 In HIC, it is standard for splints to be temporary to a circumferential cast for non-operative treatment.18 In LMIC, there may not exist resources to re-splint or re-cast putting greater emphasis on the initial splint. Therefore, to appreciate clinical success rate of these splints in LMICs, a study would need to examine outcomes after 6-8 weeks, the standard time for a fracture to heal.1
Increasing mechanical strength of plaster can be achieved by adding 10 or more layers.19 This increases the overall weight of the splint and could compress structures and decrease patient comfort.19 The increased risk of compression may not be a concern in HIC where proper training avoids this complication; however, in LMICs, there are already high rates of limb compression complications due to improper splinting.6 A heavy splinting material may exacerbate compartment syndrome and other pressure-related complications.
Plaster splints have an overall higher breakdown rate requiring removal and replacement (33% and 66% breakdown rate for plaster short arm and short leg splints, respectively, and 21% and 17% breakdown rate for fiberglass short arm and short leg splint respectively).20 Plaster has been shown to have no measurable load-bearing capabilities after water immersion. In contrast, synthetic splints (fiberglass and polyester-PU) were shown to have a 90% recovery after 24 hours of water immersion.15 Aluminum moldable splints are also waterproof.13 These data demonstrate the limitations to plaster’s potential to provide immobilization in LMIC settings where there is scarce personnel and supplies for adequate replacement.
Moldability and Flexibility
Plaster, fiberglass, polyester-PU, thermoplastics, and silicone rubber are embedded into bandages, allowing easy limb molding and splinting.9 Plaster has been found to have a more precise mold over fiberglass and polyester-PU.21,22 Fiberglass has a stiffer, more specific splint construct with better limb motion reduction than thermoplastics.23 The latter reveals the inferiority of thermoplastic splints regarding fracture immobilization relative to other commonly used materials. The aluminum moldable splint also has moldable features due to the thin strip of aluminum between the padding. However, studies are needed to examine the moldability of the splint compared to other materials. Silicone rubber is a very flexible splint due to the elastic properties of the silicone polymers and is almost exclusively used for on-the-field sports injuries.11
Ease of application
Splinting materials suited for LMICs should have an innate ease of application for easy training. The ease of application can come from the physical properties of the material such as activation heat requirements, setting time, curing time, load-bearing time, and toxicity.
Parmar et al. evaluated the use of plaster casting and concluded applying a plaster splint to be “messy and cumbersome” due to the extra layers required for adequate strength24 and can take over 20 minutes to apply.20 This conclusion is consistent with other reviews examining application. Polyester-PU is applied similarly to plaster in layers of bandages and can be challenging to apply due to a firm adherence to the skin.9 Fiberglass offers a cleaner application due to the lack of paste and fewer layers, however, must be applied with gloves due to skin toxicity.9 Thermoplastics and Woodcast require high temperatures for molding done by trained personnel to avoid thermal damage.9 Silicone rubber splints require training to pour the silicone into the desired limb mold.11 In contrast, aluminum moldable splints are immediately molded to the patient’s limb without the use of extra materials, water, gloves, or hardening time. This may be ideal for LMIC use with limited training, though their long-term durability remains under-studied.
It has been found that the error rate of splinting is significantly higher in non-orthopaedic providers applying splints in a HIC.25 In this study the providers are board certified HIC physicians, therefore this gap is expected to be even higher in LMICs where splinting is completed by personnel with minimal formal training hence emphasizing the need for easy application.
Availability/Cost
In Ekanayake et al.'s 2023 review, plaster was ranked the cheapest, followed by silicone rubber, thermoplastic, fiberglass, PU resin, and Woodcast as the most expensive material per package.9 Other studies found fiberglass to be 2-3x more expensive than plaster. Comparing the cost of 30cm of material (the average length of a short arm splint) from one distributor, plaster is $1.05, aluminum moldable splint is $1.31, fiberglass is $1.64, polyester-PU is $1.94, and thermoplastic is $42.19.26–28 Plaster and aluminum moldable splints are the most cost effective. With aluminum moldable splints retailing for $3.99 for 36in28 and aluminum costing $2.61 per 1 kg,29 it is reasonable to assume they can be manufactured at a low cost. The same is true for plaster splints. With manufacturing accounting for 82% of the developing-world’s employment, the developing world seeing more medical manufacturing since the COVID-19 pandemic, and high unemployment rates within LMICs, there is the potential and resources for these products to be manufactured within LMICs at an economical benefit.30,31
These results are summarized in Table 2. This analysis has shown each material’s limitations to its use in LMICs and demonstrates the need to examine further alternative splinting materials that minimize these limitations.
DISCUSION
To date, there is no literature that discusses the ideal splinting material for MSK injuries in LMICs. The purpose of this review was to examine the common splinting materials according to four common goals identified for the intended purpose to be used in LMICs. LMICs differ in their infrastructure, training, and supplies and therefore it cannot be assumed that materials used in HIC align with the needs in developing countries.
Plaster is a widely used splint material yet has many limitations to its widespread use in LMICs. The ease of application, specifically the number of layers required for adequate strength, could exacerbate risk for compartment syndrome in LMICs. Potential plaster breakdown is less conducive to a LMIC setting where supplies and medical training are limited for adequate replacement. Additionally, plaster splints are one-use splints and have been shown to have the highest emission of greenhouse gases during disposal and human cancer toxicity compared to fiberglass and resin,32 an important consideration in LMICs where waste management infrastructure is limited.33
Fiberglass splints eliminate some of the limitations posed by plaster. They are not applied as a paste, do not require layers, and have shorter setting times streamlining the application process which may be conducive to an LMIC with a high demand for care. Although fiberglass has a higher intrinsic strength, the cost is a limiting for use in LMICs. Polyester-PU and thermoplastics are ill-suited for LMICs for similar reasons—high cost and application challenges. Silicone rubber is not a practical splint by design. Woodcast is biodegradable, has a straightforward application, short setting time, decreased risk of thermal damage, and good intrinsic strength and moldability, but it is not cost-effective for LMICs. Aluminum moldable splints may eliminate the limitations associated with plaster such as requiring only one layer of aluminum, lack of paste, no water associated damage, and nonbrittle material. These splints are multiuse and could eliminate some of the environmental concerns in waste management with plaster splints, a potential benefit for LMICs. Yet, the lack of biomechanics research on the structural integrity of the splint makes it challenging to recommend widespread use.
Of the splints reviewed, plaster and aluminum moldable splints have several benefits and minimal disadvantages for LMIC use, including total cost. Mass roll out of these splint materials may be challenging from a legislation perspective and high initial overhead costs of manufacturing; however, they have the potential to reduce total costs of musculoskeletal care. For example, in Malawi an inpatient stay for a radial and ulna shaft fracture costs a total of $237 to $621 with proximal ulna fractures costing upwards of $900.25 By implementing a standard splinting material in addition to more formal educational programs in LMICs, there is the potential to avoid splinting complications and increasing successful non-operative fracture treatment to avoid these costly inpatient stays. In this example, a $3.99 reusable splint (aluminum) or $1-2 disposable splint (plaster) could reduce overall economic burden of musculoskeletal care.
This study has several limitations. A qualitative literature review is subject to availability bias given that some materials are more frequently studied than others. Additionally, many of these materials are available through multiple medical company venders and distributors making it challenging to find an accurate representation of cost for comparison.
CONCLUSIONS
Out of the standard splinting materials, plaster was found to be the most cost-effective yet has limitations to its widespread use in LMICs. Fiberglass silicon rubber, polyester-PU resin, thermoplastics, and Woodcast are not cost-effective for LMIC use or have significant challenges in application ease. Aluminum moldable splints may solve some of the issues presented with plaster and the issues of cost with other materials, but further research is needed to assess their clinical efficacy and accessibility for use in LMICs.
This review identified two potential splint materials for use in LMICs, plaster and aluminum moldable. An appropriate follow up study is to assess the feasibility of these splints in the context of LMICs, either with a small randomized controlled trial or focus group. Various LMICs and settings (rural versus urban) should be considered to account for country-specific splinting challenges. Additionally, further initiatives to decrease splinting complications in LMICs could include education with development of a splinting course, collaboration with local partners, and working directly with community members in LMICs.
Funding
None
Authorships
All authors contributed equally.
Competing interests
The authors completed the ICMJE Disclosure of Interest Form (available upon request from the corresponding author) and disclose no relevant interests.
Correspondence to:
Brianne M. Giuffrida, BS, BA, Department of Orthopaedic Surgery, Drexel University College of Medicine, 60 N. 36th Street, Philadelphia, PA 19104; e-mail: bmg332@drexel.edu