BACKGROUND
Improving sexual and reproductive health (SRH) is a key strategy for reducing health disparities worldwide.1 Goal 5 of the SDGs is to achieve gender equality and empower all women and girls. The related Target 6 is to ensure universal access to sexual and reproductive health and reproductive rights by 2030 in accordance with the Programme of Action of the International Conference on Population and Development (ICPD) and the Beijing Platform for Action.2,3 Achieving this SDG target remains the responsibility of all countries tasked with tracking their country level progress towards this target.
An important indicator for tracking national progress toward this target 5.6 is Indicator 5.6.2. which measures the “Number of countries with laws and regulations that guarantee full and equal access to women and men aged 15 years and older to sexual and reproductive health care, information and education”.2 This indicator was prioritized as a core indicator in the monitoring framework for the Ending Preventable Maternal Mortality (EPMM) Strategies.4 This was because of its potential to drive progress towards Key Theme 1, which focuses on empowering women, girls, families and communities in the specific context of maternal health. The prioritization was based on the fact that this indicator is fundamentally linked to all SDG’s and ensures an enabling environment for Sexual Reproductive Health Rights (SRHR).5 Through the policy level domain of SRHR, SDG 5.6.2 attempts to operationalize human rights measurement.2
To measure SDG 5.6.2, the UN 12th Inquiry module, a self- reported survey tool for counties to be completed by their governments and relevant ministries or departments was developed under the direction of the United Nations Population Fund (UNFPA). The tool was piloted in 2017. Thereafter, a call was put out to governments of countries, to provide the baseline data as part of their commitments towards achieving the SDG indicator. This was to be done by filling out the UN 12th Inquiry module tool starting from 2018.6,7 However, as of December 2019, only 107/195 (55%) countries had submitted data on the SDG 5.6.2 indicator.2 The UN raised concerns about unresponsiveness from countries to provide data on targets and indicators, leading to difficulty in tracking global progress toward the SDGs.2 This in turn, led to difficulty in identifying areas in the SDG indicator that need the most attention, and jeopardized collective achievement of the global goals and targets.6,8 Ghana was among the countries that had not yet provided baseline data on SDG 5.6.2 to the United Nations (UN) as at June 2019. As a country which has committed to ensuring that SRHR of all members of the country are maintained through policy implementation in spite of socio-cultural barriers,9 there is the need to periodically track the county’s progress.
As part of efforts to improve maternal health measurement capacity and use, ten indicators on maternal health were selected for systematic research to assess their validity in a multi-country study carried out in Ghana, Argentina and India. In Ghana, SDG 5.6.2 was prioritized as an indicator for validation by the Ghana Health Service and key maternal health stakeholders in the country. In order to enable that process, the research team facilitated the process for completion of the UN 12th Inquiry Module survey. We detail here the process and outcome of documenting Ghana’s progress towards achieving SDG 5.6.2 .
METHODS
Overview of Ghana
Ghana is a middle-income country located on the west coast of sub-Saharan Africa. The country has a population of over 30 million people with approximately 720,000 women of reproductive age.10 The country has a health system that places priority on maternal healthcare.11 In 2008, the government of Ghana announced a free maternal health care policy to enable pregnant women to access an essential comprehensive maternal healthcare package.12–14 All health-related activities in the country are led by the Ministry of Health.
Data collection tool (The UN XII Inquiry module)
Data was collected using the SDG 5.6.2 official tracking tool which is the “UN 12th (XII) Inquiry Among Governments on Population and Development, Module II on Fertility, Family Planning and Reproductive Health”.15 The tool contains a total of 33 questions which collect information on legal enablers and barriers in the forms of laws, policies and regulations on SRH environment in the country and is expected to be filled out by each country. This information is then compiled across four broad parameters of sexual and reproductive health and rights (SRHR), namely, maternity care, contraception, comprehensive sexuality education, and sexual health and wellbeing with the four sections further divided into 13 components (Table 1). Table 1 shows the four broad sections with their respective components and the specific areas of SRH they each cover.
After completing the survey, a national validating team made up of the Government, United Nation Country teams, and civil society organizations are expected to review the filled form for multiculturalism or inclusiveness of all groups of people in the country.16 The completed survey for each country was expected to be submitted to United Nations Population Fund (UNFPA) by December 2018 for review, analysis and monitoring of the global progress towards achieving the SDG goal.17 In the same way, this survey tool was used to collect all the information available on the SRH in Ghana covering the 4 broad sections with their 13 components.
Participant’s Involvement and Data collection (Consultation process)
We conducted an exhaustive desk review of all publicly available national and subnational laws, legal statutes, regulations, executive orders, decrees and ordinances. In order to ensure completeness of all available documentation, we consulted with Ghana Health Service (GHS), Ministry of Health (MoH) and other health stakeholders in Ghana and conducted key informant interviews with them.
We also engaged staff from the MoH, GHS and United and UNFPA to support data collection and obtain the list of the key stakeholders in maternal health for a broader stakeholder engagement meeting to validate the survey responses and discuss their implications.
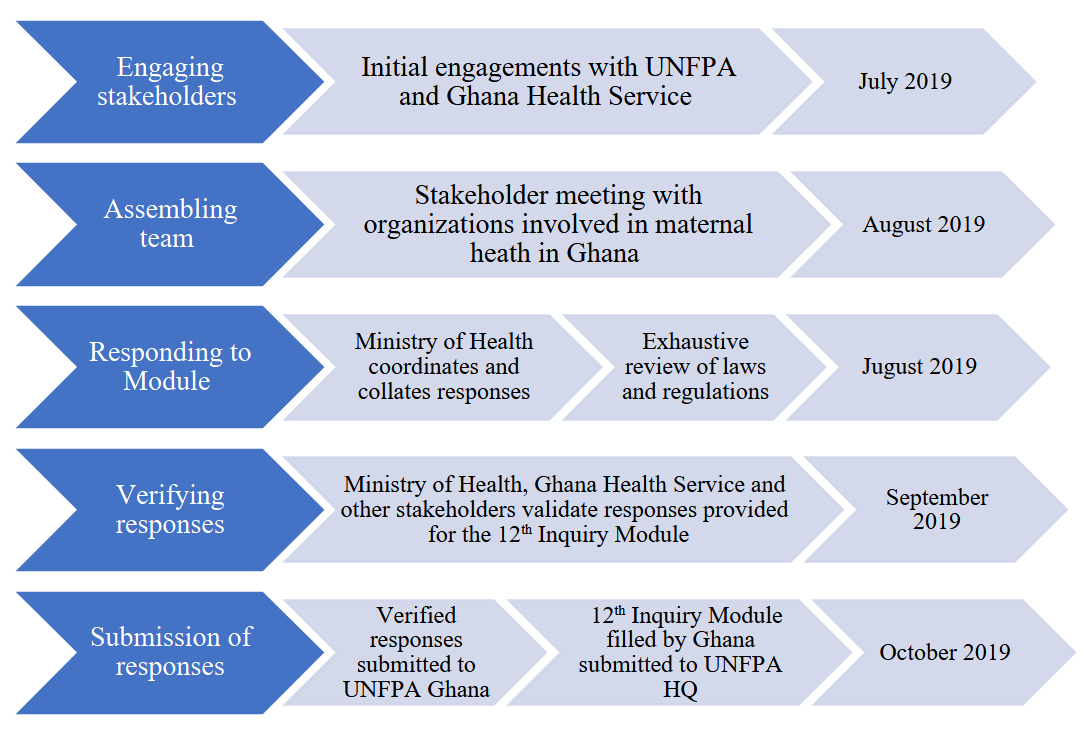
We then convened a formal technical consultation meeting in collaboration with the identified key stakeholders in the form of a focus group in July 2019. Participating stakeholders were from the UNFPA, the World Health Organization (WHO), United Nations International Children’s Emergency Fund (UNICEF), Ghana Coalition of NGO’s in Health, Planned Parenthood Association Ghana, National Health Insurance Authority, Christian Health Association of Ghana, National Catholic Health Services, Ministry of Health, Ghana Health Service, Society of Obstetricians and Gynaecologists of Ghana (SOGOG), Ghana Registered Midwives Association and the Paediatric Society of Ghana. The meeting focused on discussions to obtain any additional information relevant to SDG 5.6.2 to supplement the responses to the UN 12th Inquiry Module II survey. Stakeholders were taken through the survey questions and agreed to provide the needed information from their institutions for this purpose. Further, stakeholders deliberated on the relevance of the SDG 5.6.2 target and the need for tracking its progress in Ghana.
The Ministry of Health was tasked to coordinate the process of finalizing the filled 12th Inquiry Module with assistance from UNFPA Ghana. The Ghana Health Service was assigned with the responsibility of working closely with MoH to ensure that adequate responses were provided for the country. All other stakeholders were responsible for providing information from their organization that was pertinent for completion of the survey. The University of Ghana School of Public Health coordinated the process, convening stakeholders and following up via phone calls, emails, and in-person meetings to ensure that all responses were obtained from the relevant ministries and organizations and all data were compiled for inclusion in the final survey submission. Finally, the MoH submitted the final version of the survey in October 2019 to the UN on behalf of the country. Figure 1 provides a pictorial summary of the process.

Data Analysis
Survey data collected were analyzed using the UN SDG 5.6.2 original scoring approach. Scores were calculated for each of the 4 sections using the respective components in the section. In all, there were 13 components of SRHR divided across the four sections respectively.
For each component, scores were calculated using legal enablers and barriers. The number of enablers present was divided by the total enables in the component. Similarly, the number of barriers present was divided by the total number of barriers in the component.
-
Each component was scored independently and weighted equally
\[ S i=\left(\frac{e i}{E i}-\frac{b i}{B i}\right) \times 100 \]
-
Where:
-
𝑆𝑖: Score for component i
-
𝐸𝑖: Total number of enablers in component i
-
𝑒𝑖: Number of enablers that exist in component i
-
𝐵𝑖: Total number of barriers in component i
-
𝑏𝑖: Number of barriers that exist in component i
-
A section score was calculated as the arithmetic mean of the constituent component scores for a given section. The total score and the four section scores were reported as percentage scores between -100 and 100, reflecting the extent to which laws and regulations exist to guarantee full and equal access to sexual and reproductive health care, information, and education. A total indicator score was calculated as the arithmetic mean of the13 component scores.
The outcome of the stakeholder engagement meetings and Ghana’s scores from the completed survey were presented in narratives and charts and text.
RESULTS
A total of 15 key maternal health stakeholders from public and private organizations in Ghana were engaged in completion of UN 12th Inquiry, Module II.17 Based on responses from the FGDs and KIIs enablers and barriers of SRHR were used in filling out the survey, Box 1 displays the responses used to calculate the component and section scores for Ghana.
Ghana’s score for the 12th Inquiry Module
Following the computation of the value of the indicator, Ghana had a total score of 73% (Table 2). The four section scores ranged from zero (0) for Section 3, indicating no evidence of laws on “comprehensive sexuality education and information”, in Ghana, to 100% for Section 2 which covers “contraception and family planning” (Table 2).
DISCUSSION
This paper documents Ghana’s process of data collection and analysis to track progress made towards achieving SDG 5.6.2. Countries were expected to provide updates on their progress towards achieving SDG 5.6.2 to the United nations through a survey by the UNFPA by 2018; however, 36 countries including Ghana were unable to meet this deadline.2 Completion of the national survey required information sharing and coordination among the various Reproductive and Sexual Health Service (RSHS) stakeholders in Ghana with leadership from the GHS, MoH, and UNFPA. The success of this process highlights the importance of strong country ownership and effective collaboration among public and private stakeholders working together to achieve a common good for the benefit of the nation.
Assessing the country’s scores section by section and reviewing all components, the scoring suggests there is evidence of barriers to contraception and family planning (S2). This is an indication that Ghana’s laws and policies related to contraception provide an enabling environment that guarantees citizens access to family planning. This is consistent with recent implementation of a number of programs aimed at improving access to sexual and reproductive health care to all populations in the country.18,19
Similarly, the survey results reflected a high score in Section 1, Maternity care, but with a barrier in access to abortion. Although laws on safe abortion are evident in Ghana, some clauses included in these statutes are considered as barriers to this service based on the SDG assessment criteria. This implies that the people who need the service may be hindered by the current SRH environment.
Low scores received on specific components such as S3: Comprehensive Sexuality Education (CSE) and Information were largely due to the absence of either laws or policies which would serve as enablers or barriers to access for the SRHR guarantees described in those sections of SRH.
Overall, the high score obtained on the UN Inquiry 12, Module II survey suggests the SRH environment in Ghana is quite good. Ghana’s score reflects achievement of 73% progress toward an enabling environment reflected in laws and regulations indicates that the SRHR of the people in Ghana is of importance to their government decision makers. However, the scores of the individual sections point out the need to focus on implementing laws and policies which reflect each of the specific areas within the SRH environment in the country.
A close look at the scoring for the indicator raises a few concerns that could be interrogated further. For example, the computational method for scoring the indicator subtracts barriers from enablers, but does not take into consideration the absence of laws which may be essential for the SRH environment. Ghana received no score for Section 3 (Comprehensive Sexuality Education (CSE) and Information) due to the absence of laws or regulations governing CSE in Ghana. Although some guidelines on CSE exist and are being implemented in parts of the education sector, they have not been developed into policies and laws with national scope.20,21 This situation is similar to what was reported in the SDG 5.6.2 baseline global report, comprising the data from countries that had responded to the module at the time of its publication, when CSE was identified as a gap for more than half of the countries that completed the survey.2
This highlights the importance of disaggregating the indicator data for its interpretation as countries move toward achieving the 2030 target. Taking into account the overall score alone may not portray the full picture of the SRH environment in Ghana, or any given country. For meaningful action to address gaps, focus should also be placed on the component and section scores that need to be addressed to meet the 2030 target.
In addition, periodic tracking of the progress being made is imperative to ensure countries are not losing focus. Innovative measures for tracking at the global, regional and country levels are required to be able to achieve the goal of gender equity by 2030.22
The major challenge encountered in completing the UN 12th Inquiry, Module II was in bringing together stakeholders for discussions and obtaining the necessary information, resulting in delays. The process required collaboration between the UNFPA country offices, Ministries of Health and other relevant government institutions. Effective coordination by a third party to bring the stakeholders together and capture the required data was required to overcome this challenge. The need to build stronger intersectoral collaboration was the main lesson learned from this process, underscoring that timely information-sharing can be accomplished through collaboration. The process was coordinated by a team of external facilitators but the survey was completed by the Ministry of Health per UNFPA instructions. To reduce respondent bias, responses were verified against existing documents and both responses and data sources validated.
CONCLUSION
Ghana fulfilled the UN request to complete the 12th Inquiry Module II. This allowed the national progress and global comparisons of the SDG 5.6.2 to be tracked. The outcome was achieved through collaborative efforts from Ghana Health Service, Ministry of Health, UNFPA and other relevant organizations, with coordination and facilitation from the University of Ghana School of Public Health provided with support from the Improving Maternal Health Measurement (IMHM) Project of the Harvard T. H. Chan School of Public Health.
The outcome of Ghana’s survey suggests significant national progress toward SDG 5.6.2. reflecting an enabling policy environment and laws and regulations that are 73% able to guarantee full and equal access to women and men aged 15 years and older to sexual and reproductive health care, information and education. Though some sections reflect fully guaranteed access, direct efforts should be made towards improving laws and policies on full and equal access to CSE overall, and to specific components of the SRHR environment such as access to the HPV vaccine where there are currently no laws or regulations.
To enable countries to strengthen available measures and monitoring efforts to meet this SDG target and others, we recommend stronger intersectoral collaboration and facilitation of information sharing to achieve the goal.
Acknowledgements
We acknowledge the following stakeholders for their time and support during the activity; United Nations Population Fund (UNFPA), the World Health Organization (WHO), United Nations International Children’s Emergency Fund (UNICEF), Ghana Coalition of NGO’s in Health, Planned Parenthood Association Ghana, National Health Insurance Authority, Christian Health Association of Ghana, National Catholic Health Services, Ministry of Health, Ghana Health Service, Society of Obstetricians and Gynaecologists of Ghana (SOGOG), Ghana Registered Midwives Association and the Paediatric Society of Ghana and the data extraction team. We also acknowledge the entire IMHM Team from Boston, Argentina and India from their support during the project.
Ethical statement
We received institutional review board approval from Harvard University (approval ID: IRB19-1086). In Ghana, the study was approved by the Ghana Health Service Ethical Review Board (approval ID: GHS-ERC022/08/19). Additionally, permission was obtained from all required national and sub-national government health authorities to carry out the study. Written informed consent was obtained from all study participants before the surveys were administered. Data were stored using level IV Harvard security measures, including use of Harvard REDCap for data management, locked and secure data storage facilities, and encrypted data storage devices.
Data availability
The datasets used and analysed during the current study are available from the corresponding author upon reasonable request.
Funding
This work was supported by the Bill and Melinda Gates Foundation through an award to RRJ and AL (Improving Maternal Health Measurement (IMHM) Capacity and Use, grant number OPP1169546). Funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Authorship contributions
DAB, EK, MO, RA planned and executed the meeting stakeholder meetings. All authors contributed intellectually to the conceptualization, implementation, and interpretation of the meeting results, participated in drafting the manuscript, and reviewed and approved the final version.
Disclosure of interests
The authors completed the ICMJE Declaration of Interest Form (available upon request from the corresponding author), and declare no conflicts of interest.
Correspondence to
Delia Akosua Bandoh, School of Public Health, University of Ghana, P.O Box LG 13, Legon, Accra, Ghana deliabandoh@gmail.com