INTRODUCTION
Severe neonatal hyperbilirubinemia (SNH) is a common problem in low- and middle-income countries (LMICS), especially in Sub-Saharan Africa, with 667.8 cases and 186.5 exchange transfusions (ET) per 10,000 live births, compared with 4.4 cases and 0.38 ET per 10,000 live births in the Americas.1 Delayed care-seeking may result in avoidable ET, bilirubin encephalopathy with long-term disability and even death.2 A Blended Learning Quality Improvement Program was developed between Georgetown University Medical Center (GUMC), MedStar Georgetown University Hospital (MGUH) and eight district and small regional hospitals in Ghana to improve the quality of level II neonatal care, applying the WHO SEARO Point of Care Quality Improvement approach.3 Prevention of SNH was chosen by two of the hospitals as a pressing problem and is reported here.
Understanding the Problem
In Ghana, about 88% of women deliver in health care facilities.4 The Ghana Health Service recommends keeping low-risk, mother- baby dyads for 24 hours, but many are discharged within a few hours after birth, due to overcrowding or parents’ wishes.5
Checking bilirubin levels prior to discharge is not practiced. A number of newborns who subsequently develop jaundice at home are brought back late with SNH requiring exchange transfusion to prevent kernicterus.
Exploring reasons behind Problem
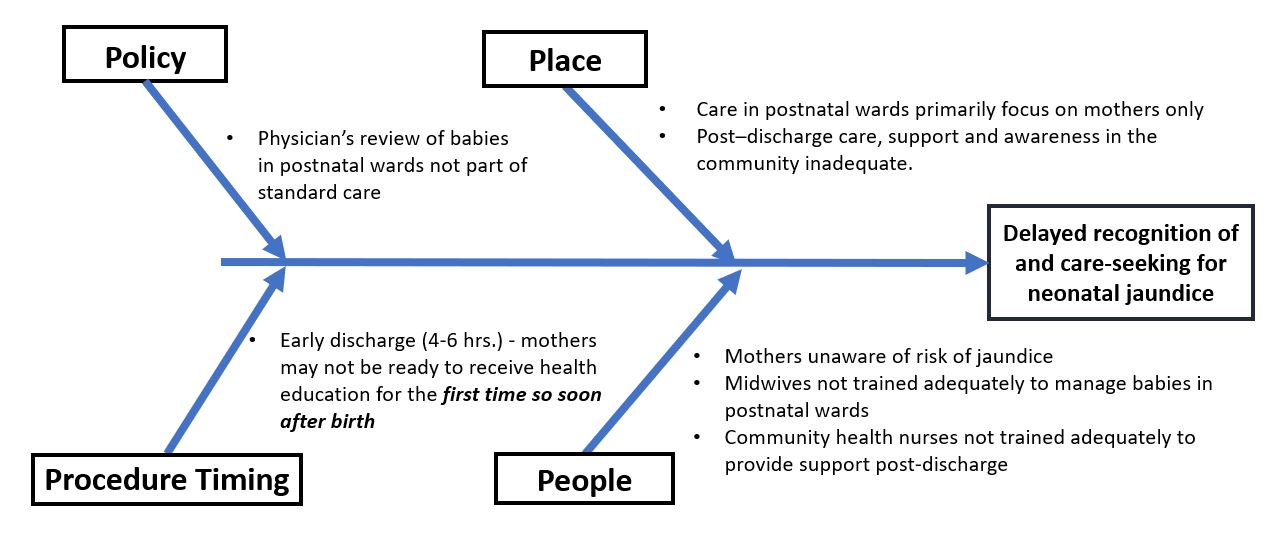
In determining reasons for delayed care-seeking, focus was laid on issues that could be rectified through interventions that were feasible with existing resources within the individual hospital using the “fish bone analysis” (Figure 1).

METHODS
A national-level workshop was planned on key topics specific to level II neonatal care, combined with follow-up facilitation through digital technology, focusing on quality improvement activities on topics chosen by individual hospitals. Digital technology included the use of a video communication platform, teleconferencing (Zoom for the main interaction, WhatsApp for quick messages and for promoting local interaction; and a cloud storage service, Google Drive for sharing documents and surveys), managed by the authors (IN, JR and JKA). Due to the COVID-19 pandemic that commenced shortly thereafter, the workshop was cancelled, but distance learning activities were continued. These included small group sessions on individual facility quality improvement (QI) activities weekly or biweekly, as required. Monthly two-hour academic sessions included case presentations, sharing of QI results and discussions on selected technical areas by staff from the Division of Neonatal Perinatal Medicine, MGUH, and Ghana health care providers. The Georgetown University Institutional Review Board declared the study to be exempt from review. Permission was taken from hospital administrations to share data redacting patient identifiers. This study focusses on SNH chosen by two hospitals.
SMART aims at the initiation of the study
(a) To increase by 15%, within 3 months, the proportion of inborn newborns ≥ 34 weeks gestational age who develop jaundice after discharge being brought back early to the hospital within 72 hours after birth; and
(b) To reduce median bilirubin levels, at readmission, of inborn babies ≥ 34 weeks gestational age, by 10% in 3 months
It may be noted that the above aims turned out to be inappropriate and were revised for reasons explained below in the results section.
Interventions implemented
Interventions were focused on inborn newborns ≥34 weeks’ gestation. Out-born and inborn preterm babies < 34 weeks who had longer stays in the neonatal unit were excluded. Although conventionally the Plan-Do-Study-Act (PDSA) cycle system recommends testing individual actions one step at a time, it was found to be more practical and less time-consuming to implement several activities simultaneously, since it was clear from the beginning that multiple components needed to be addressed.3 Key processes included:
-
Formation of QI teams with continued advocacy for regular meetings.
-
Review and, where needed, adaptation of tools (posters and videos) for early postnatal counselling of mothers.6,7 Counselling on jaundice was incorporated into the general health education on basic care of the baby.6 Based on local practice, mothers were requested to bring back babies whenever they noticed jaundice, regardless of whether the jaundice reached a particular body part.8,9
-
Training of midwives for implementing interactive health education in the postnatal ward. Emphasis was laid on the interactive nature of counselling sessions. A midwife had to be present at least once a day during screening of health education videos, pausing it intermittently to highlight key points. Mothers were asked to simultaneously look for the various signs in their babies to facilitate similar actions after discharge. The midwife randomly requested one or two mothers to demonstrate some of the steps to ensure that they had understood key issues. Refresher training of midwives was instituted on a six-monthly basis.
-
Initiating daily rounding in the postnatal ward by a physician from the neonatal unit in Hospital A. Hospital B already had daily rounds by a neonatal unit physician.
-
Informing relevant community-based community health nurses (cCHNs) for follow-up. Facility-based midwives were requested to contact cCHNs in the localities where the mothers were planning to spend the postnatal period, to provide contact details to promote calls and plan home visits.
Selection of indicators
Based on existing local challenges, including limited staff and the onset of the COVID-19 pandemic, the focus was on essential outcome indicators/measures. Although valuable to discern fidelity and good clinical practice, process indicators were not individually measured.10 Team leads were, however, requested to periodically verify that the activities were implemented through conducting random spot-checks. The outcome measures addressed serum bilirubin level at admission and number of exchange transfusions (ET). Hospital A relied on serum bilirubin for assessing neonatal jaundice. Hospital B often used the transcutaneous bilirubinometer, as blood samples had to be sent to a neighbouring laboratory, resulting in delays. Decisions for interventions in Hospital B were thus, on occasion, based entirely on transcutaneous bilirubinometer readings.
Data collection
A quantitative longitudinal approach was used, analyzing data monthly and focusing on differences observed during the pre-intervention (October 2019 through December 2019) and post-intervention (January 2020 through May 2021) phases. Participating hospitals used pre-designed Excel spreadsheets to collect raw data.
Data analyses
All variables obtained were described as frequencies and percentages for categorical variables and presented as a line graph to observe trends over months. Data for each hospital, verified by unit heads, was carefully reviewed and analyzed primarily by the external facilitating team member (JKA) using SPSS version 27.0. Data for each hospital was analyzed separately and not cumulated together as the hospitals differed in size and patient population. Results were never compared between the hospitals, but they were able to see each other’s data to discuss best practices, promoting peer learning.
Review and sharing of results
Through virtual meetings, results were discussed among external facilitators, lead persons of the participating hospitals, and other QI team members to encourage active participation, identify bottlenecks, and plan additional interventions as required. These smaller group sessions were organised multiple times, at times weekly. The larger monthly meetings involving other interested hospitals also served to share results and lessons learnt on QI activities with the whole group.
RESULTS
Hospital A is a public district hospital, with 3000 deliveries in 2020. The 30-bed level II neonatal unit operates as a “Mother and Baby Unit” (MBU) caring for in-born and out-born at-risk, small and sick babies up to the age of 2 months, kept together with their mothers. The MBU, distinct from the post-natal ward, had 1190 babies admitted in 2020. Hospital B is a faith-based district hospital run by a quasi-government agency, with 2193 deliveries in 2020. It has a conventional 34- bed level II neonatal unit with the babies kept separate from their mothers, with 925 admissions in 2020.
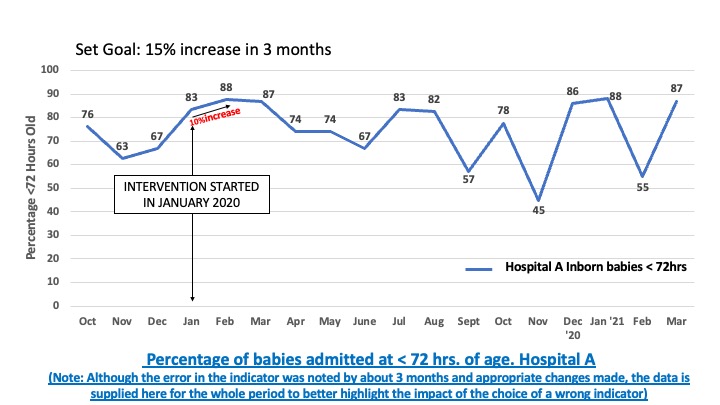
Run charts were developed and monitored, indicating proportions of inborn babies with jaundice being brought in for re-admission within 72 hours of age and median bilirubin levels. On review, trend lines fluctuated over the months but did not show results that could be interpreted in any meaningful manner, especially related to quality improvement issues. (Figure 2).
.jpg)
Based on the unclear trend graph, QI teams reviewed the interventions through a troubleshooting process summarised in Table 1.
It soon became clear that there was a need to identify a more meaningful outcome measure. Based on careful re-evaluation and discussions with the teams, it was modified to proportions of babies admitted with pre-defined thresholds of bilirubin, namely (a) ≥ 340 µmol/L (≥ 20 mg/dL) -high level, (b) ≥ 255 µmol/L (≥ 15 mg/dL.) to ≤ 339 µmol/L (≤20 mg/dL) – moderate level and (c) ≤ 255 µmol/L (≤ 15 mg/dL) - low level.
The SMART aim was revised as noted below:
(a) To increase by 15%, within 3 months, the proportion of discharged inborn newborns ≥ 34 weeks gestational age who were brought back to the facility for jaundice, with bilirubin levels that permitted timely phototherapy to avoid SNH and ET.
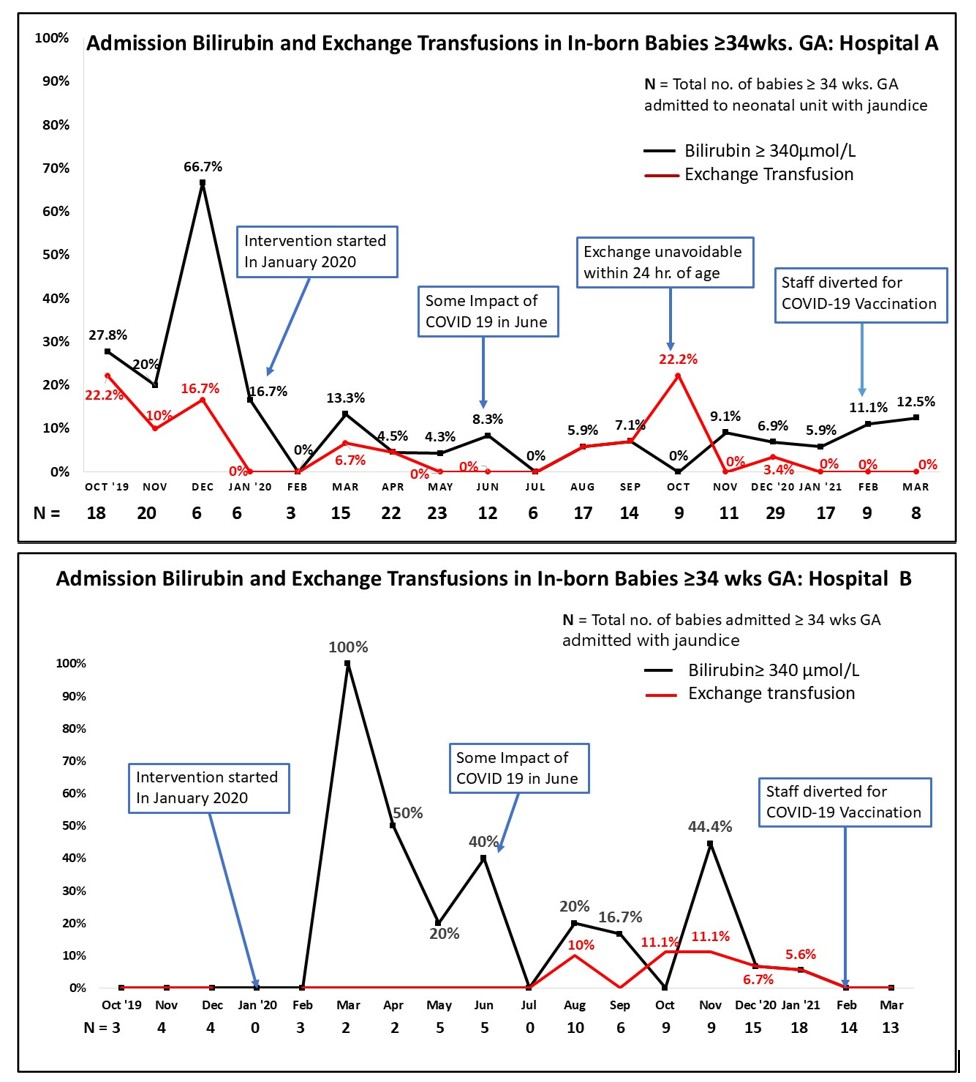
With revised outcome measure, results became more meaningful (Table 2 and Figure 3).
_and_b_(below).jpg)
In Hospital A, the percentage of babies admitted for SNH (>340 µmol/L) dropped by 77.4%, and ETs dropped by 67.8%. The two ETs carried out in Hospital A during October 2021 on twins were unavoidable, being due to severe ABO hemolytic disease. (Fig. 3). Following QI interventions, the proportion of babies brought with bilirubin levels > 20 mg/dl decreased by 31.3 % in the first 3 months. The fall was mostly sustained (by 32.5% even after 13 months). There were some periods when the improvement observed was less, as in February and March 2021, where there was a shortage of staff either due to their contracting COVID-19 or being redeployed for other related work, including administering vaccines. Percentages varied over the year, but remained below the pre-intervention levels.
Hospital B reported having several admissions of babies with SNH and performed a number of ETS earlier, but, unexpectedly, in the 3-month pre-intervention period, no babies were admitted with high bilirubin levels and no ET took place (Figure 3). In the immediate post-intervention phase, there were babies who were admitted with high bilirubin levels (>340 µmol/L) needing ET, resulting in erratic results. Further, with fewer patients, it was noted that even one case coming in with high levels resulted in as much as a 50% change, skewing the trend graphs. From August 2020, the inborn re-admissions for jaundice were relatively higher, with more babies being brought in early with lower levels of bilirubin. In November 2020, there was again a spike in babies with high levels of bilirubin, attributed to fewer available staff due to COVID-related issues. With the reinstatement of QI activities, results again improved.
Balancing Measures (Unintended Consequences)
The percentage of newborns brought back with bilirubin levels < 15 mg / dl doubled in Hospital A. This posed additional challenges as not all required phototherapy. Where the parents resided close to the facility, they were asked to return the next day for reassessment. Those having transport problems were admitted for observation. This often led to parents being dissatisfied that their babies, kept for observation, were getting “no treatment”. Additional counselling helped to address this issue.
Virtual interactions
Virtual interactions were found to be very useful for facilitating QI processes, especially during the COVID-19 pandemic, permitting frequent interactions between both small and large groups, even on a weekly basis, far more than what would have been feasible through in-person meetings. Fortunately, we did not face significant internet challenges as would be expected in rural areas and smaller centres, partly because we were interacting with level II units in facilities that were better situated. Within meetings, we noted that some of the junior staff tended to remain quiet, which was more challenging to pick up than in face-to-face meetings. We addressed this to some extent by requesting senior staff to encourage the participation of junior workers. WhatsApp was used primarily to send reminders about meetings. Google Drive was utilised to store and share documents and presentations, and to carry out surveys when required.
DISCUSSION
SNH is so prevalent in Ghana that the Pediatric Society of Ghana has established a “Jaundice Awareness Month”.11 A study in Ghana indicated that only 17.3% of mothers had even heard of jaundice.12 While we cannot generalize based on evaluation of two hospitals, our findings provide useful information on decreasing SNH in LMICs. Our study highlights the value of choosing appropriate indicators and interactive counselling, latter being useful in promoting better understanding in mothers/families. Initiating it during the antenatal period is particularly important as also reported by Wennberg et al, instead of counselling mothers for the first time soon after the stress of giving birth, more so in mothers who get discharged very early.13 We further recommend that counselling on all major issues relevant to newborn care, particularly in the first week of life when 75% of neonatal deaths take place, should be initiated during the antenatal period, and repeated in the postnatal period before discharge.14 Including relatives in counselling is important as they have considerable influence on maternal decision-making.15
Due to the number of required activities, implementing multiple, evidence-based steps together instead of one at a time as in the conventional PDSA approach, was found to be useful and practical, especially with fewer, over-worked staff, as it was clear from the start that a number of interventions were essential. Due to challenges outlined, concentrating on outcome indicators, ensuring through lead members of the QI teams that processes were being implemented, was found to be useful in view of the limited staff in this study.10
The balancing measure, with some babies being brought in with low levels, created problems. Balancing measures are important and need to planned for and addressed early in QI activities. They are more readily missed in some over worked, understaffed units in LMICs. One could consider using low-cost devices to assess jaundice from the blanched skin color in the community and recommending return to the facility as the jaundice spreads to the chest or the palms and soles. In the past, a plastic scale, the icterometer was found to be useful.16 More recently other options are available and could be used by cCHWs17–19 Based on challenges noted in this study with relevance to community health workers and home visits, one may even consider assessment of babies by counselled mothers using one such low-cost device.17 However, in LMICs, procuring transport and estimating time required to reach facilities pose great challenges. With relevance to problems such as SNH, it may be better to arrive early. These are all challenges that need to be highlighted during interactive counselling sessions to guide families. Expanding health education through mass media, though more costly, is also beneficial, along with appropriate training of relevant health care providers, especially where the problem is common. Challenges in estimating serum bilirubin, inadequate radiance of some phototherapy light bulbs, voltage fluctuations, and electricity failures are additional factors, requiring strengthening of relevant health system pillars.20
The numbers of cases of SNH and the periodicity of their occurrence can influence trend graphs, making interpretation more difficult, as noted in hospital B. Ultimately, it is better to promote importance of frequent monitoring and emphasis on the concept that even one case being brought in late with a high bilirubin level is one too many. It would be beneficial for each unit to audit every ET to identify those that could have been avoided.
An important challenge is dependence on transcutaneous bilirubinometers for decision making about ET. This is not recommended by American Academy of Pediatrics, although it now indicates that “local consultation” should be sought due to differences in LMICs.20,21 Pre-discharge assessment with transcutaneous bilirubinometer has been found to be useful between 24-72 hours of age.22 Considering all challenges, keeping low-risk mother-baby dyads in facilities for at least 24 hours after birth, ideally, with transcutaneous bilirubin screening and having appropriate antenatal and postnatal counselling before discharge, definitely seem to be better options.5,23
Virtual facilitation of QI activities with adequate internet connection was found to be useful and low-cost for facilitation of QI activities, avoiding needless removal of health care providers from their place of work and permitting repeated interactions. At the same time, although we could not evaluate it, we feel that a balanced blended approach as originally planned, with some in-person interactions would be a better approach.
The WHO POCQI approach of working with existing resources, without waiting for full health system strengthening is important.3 However, especially in LMIC, where the health system may not be strong, there will be significant advantages, in promoting sustainability and expansion, by, at least, advocating through appropriate agencies to look into strengthening relevant pillars. Ultimately, national level up-to date policies, ideally with a budgeted national level strategy on newborn health,5 with good leadership at relevant levels, adequate funds and avoidance of rapid turnover of trained staff, with focus on optimal implementation and adequate coverage addressing equity, are essential.
CONCLUSIONS
Appropriate antenatal and postnatal interactive health education of mothers and available relatives for promoting early detection and appropriate care-seeking for problems, including neonatal jaundice, is very useful. Facilitating health care providers through digital technology within countries and internationally is not only valuable during a pandemic, but can also be applied as a part of quality improvement activities in general. They are cost-effective and a more feasible addition/option to conventional repeated supervisory visits, on-the-job mentoring and refresher workshops. It avoids taking health care providers away from their place of work. Ideally, a blended approach with some face-to face meetings may have additional advantages.
The proportion of ETs per 1000 live births may be useful as an indicator for country health information systems as documenting serum bilirubin data may be more challenging. Within facilities, every ET should be audited to verify that it was unavoidable. Ultimately, strengthening of the health system pillars with sound national and regional strategies and policies for necessary support at all levels, improved transport with adequate support for the mother and baby and appropriate effective equipment for diagnosing and managing hyperbilirubinemia are important to achieve optimal quality of care, address equitable expansion towards universal coverage and to ensure sustainability.
Acknowledgements
The authors wish to express their grateful appreciation to the following persons for their support:
-
Representative from Stakeholders in Ghana: (a) Ghana Health Service: retired Dr. Isabella Sagoe- Moses, (b) UNICEF, Dr. Mrunal Shetye, Dr. Priscilla Wobil and (c) Ghana Pediatric Society – Dr. John Adabie Appiah, who facilitated implementation of the relevant components of the program.
-
All staff in the facilities in Ghana that supported the study in collecting data and being involved in QI activities with special mention for the following (a) Sun Treso Hospital and (b) Dormaa Presbytarian
-
Georgetown University: Dr. Siva Subramanian, Dr. Nancy Crowell, Dr. Myriam Vukovic and Students: Rachel Sansone, Michelle Du, Sohelia Forbes, Sarah Atique, Crystal Wormack, Hritikh Saride, Jessica Livney, Peyton Luiz, Rhya Evans, Shoa Moosavi, Kate Norris and Elizabeth Horak
Data availability statement
Data are available upon reasonable request. The datasets generated and analysed during the current study are available from the corresponding author on request.
Funding
The Georgetown University Global Health Initiative and UNICEF, Ghana, sanctioned funds for carrying out the national training workshop in Ghana. However, as the workshop was cancelled due to the COVID-19 pandemic, the funds were not utilised to implement the study activities. Permission was granted to use the fund for open-access publication of this article.
Authorships
Dr. Indira Narayanan conceptualised and designed the study, coordinated and supervised the virtual facilitation, wrote the draft, and later revised the manuscript. Dr. Jayashree Ramasethu gave equal input to the conceptualisation, planning, and implementation of the study and revised the manuscript. Jeffery Kodjo Arhin coordinated and supervised data collection, developed graphs, and revised the manuscript. Dr. Ashura Bakari and Dr. Elliot Akoto coordinated the study within their hospitals, supervised activities and data collection from their hospitals, and revised the manuscript.
Disclosure of interest
The authors completed the ICMJE Disclosure of Interest Form (available upon request from the corresponding author) and disclose no relevant interests
Address for correspondence
-
Indira Narayanan, MBBS, MD, FNNF, FIAP, FNAMS, Georgetown University Medical Center and Division of Neonatal Perinatal Medicine, MedStar Georgetown University Hospital,
3800 Reservoir Road, NW, Suite M3400, Washington DC. 20007 Email: in83@georgetown.edu; inarayanan6@gmail.com -
Jayashree Ramasethu, MBBS, DCH, MD, FAAP Division of Neonatal Perinatal Medicine, MedStar Georgetown University Hospital,
3800 Reservoir Road, NW, Suite M3400, Washington DC. 20007
[email: jr65@gunet.georgetown.edu phone 2024448569]