INTRODUCTION
The planet Earth is reportedly and evidently experiencing a climatic shift characterised by long-term changes in weather patterns and temperatures due to several natural and man-made influences. The climatic shift is known to indisputably pose a significant disruption to the present and future fate of plant and animal life.1,2 Despite the documented technology-related and economic-motivated benefits derived from the activities that are known to be contributing to climate change, the actual and possible effects of this shift in climate is known to cause serious and fatal health effects, including on humans.1–3 This has resulted in the climate change crisis currently being experienced on Earth.
The United Nations Development Programme (UNDP) considers climate change crisis as a serious problem.4 This is mainly due to the changing climatic patterns, including extreme and hazardous weather events, rise in sea-level, acidification of oceans, biodiversity loss, water and food insecurity and health risks, among others.4 Climate change crisis is therefore the “emergency phase” of climate change (the long-term changes in climate resulting in the warming of the earth’s atmosphere, ocean and land), characterised by extreme, irreversible and continued long-term changes in weather patterns and temperatures.2,4 This is despite the early warning signs, human knowledge and awareness about the changes and its negative consequences, and regardless of the control efforts in place.2,4 Climate change crisis naturally affects the food, water, air and environment that human life and wellbeing depends on.
The World Health Organization (WHO) identified heatwaves, excessive rainfall/floods and drought among the most common and leading climate-related causes of human death, illness and discomfort/suffering responsible for up to 90% of documented natural disasters, globally.5 Heatwaves, excessive rainfall/floods and drought have been reported as direct and indirect causes of death and diseases in human populations.1–3,5 For instance, heat stress due to heatwaves was found to be the leading cause of weather-related mortality and a major contributor in the exacerbation of underlying conditions such as mental illnesses, cardiovascular diseases (CVDs) and diabetes mellitus.2,4 Heatwaves were also found to increase transmission of some infectious diseases and the risk of accidents.2 Excessive rainfall is known to cause floods, which have been cited among the most common natural disasters, having affected over 2 billion people between 1998 and 2017, worldwide.5 Drought is known to lead to inadequate food, consequently contributing to undernutrition, overall poor health outcomes and accelerated premature death.2,3,5 Mortality and morbidity from heatwaves, excessive rainfall/floods and drought can be more complex, resulting in serious outcomes. This is due to possible co-occurrence and interaction of several natural disasters with man-made disasters in societies that are already overburdened by resource constraints, diseases and weak health systems.3,5 Hence societies can be disproportionately affected by natural disasters based on several determinants.
Key determinants for the severity of heatwaves, excessive rainfall/floods and drought on human health include individual and general socio-economic and environmental conditions.3,4 Individual factors that shape health outcomes following natural disasters include age, gender, economic status and health status.2–4 Important socio-economic and environmental determinants of health outcomes include economic status and adaptation, public safety and health system strength, geography (location, severity and frequency of the EWE) and level of exposure (exposure, vulnerability and risk of occurrence).4
Though there are several documented serious and fatal health effects linked to the prevailing and alarming climate change crisis, there is limited research on the harmonised interlinkage between extreme weather events (EWEs), their effects on human health and health inequalities and response capacity mapping. Most studies were generally either restricted to effects of particular EWEs on selected health conditions or were silent on response capacity evaluation and related gaps. The study sought to scope literature on existing research evidence concerning the effects of EWEs namely, heatwaves, excessive rainfall/floods and drought on human health and health inequalities, discussing the observed determinants, patterns, interventions (where mentioned) and existing adaptation gaps serving as critical lessons for informing future preparedness and response efforts.
METHODS
A scoping review was conducted, employing a Boolean strategy to search for relevant peer-reviewed articles in electronic databases. These included Google Scholar, Scopus, websites for United Nations agencies, for example World Health Organization (WHO) and the United Nations Development Programme (UNDP). Additional sources included electronic databases for climate and health sciences such as MEDLINE and ProQuest. The search strategy was complemented by a manual search for additional relevant articles from reference lists of the already included articles.
Key terms included in the search syntax included: (Health effects/consequences OR Climate-sensitive Diseases OR Effects) AND (Determinants OR Factors OR Inequalities OR Patterns OR Interlinkages OR Relationships) OR (interventions OR Solutions OR Measures OR Disease Surveillance OR Adaptation) AND (Climate change crisis OR Heatwaves OR Excessive rainfall OR Floods OR Drought OR Extreme Weather Events) AND (Victims OR vulnerable populations) AND (Africa OR Asia OR Australia/Oceania OR Europe OR North America OR South America) AND (2025 OR before 2025) in various combinations. A modified PICOTS (Population/patient, intervention/variable, comparison/control, outcome/objective, time frame and setting/context) framework was used as a reference for the formulation of study questions and search syntax.6–8
The study considered peer-reviewed articles written in the English language and published before February 2025. Eligible studies must have investigated and reported mortality and/or health effects of at least one of the exposures of interest, which are heatwave, excessive rainfall/floods and drought in defined human populations.
Articles that did not specify the study objective(s), study design, EWE and EWE-related health effect(s), study location and study year were excluded from the final analysis. Additionally, abstracts, review manuscripts, letters to the editor or those that did not meet the required quality were excluded. Articles with restricted institutional/payment access could also not be included in the final analysis.
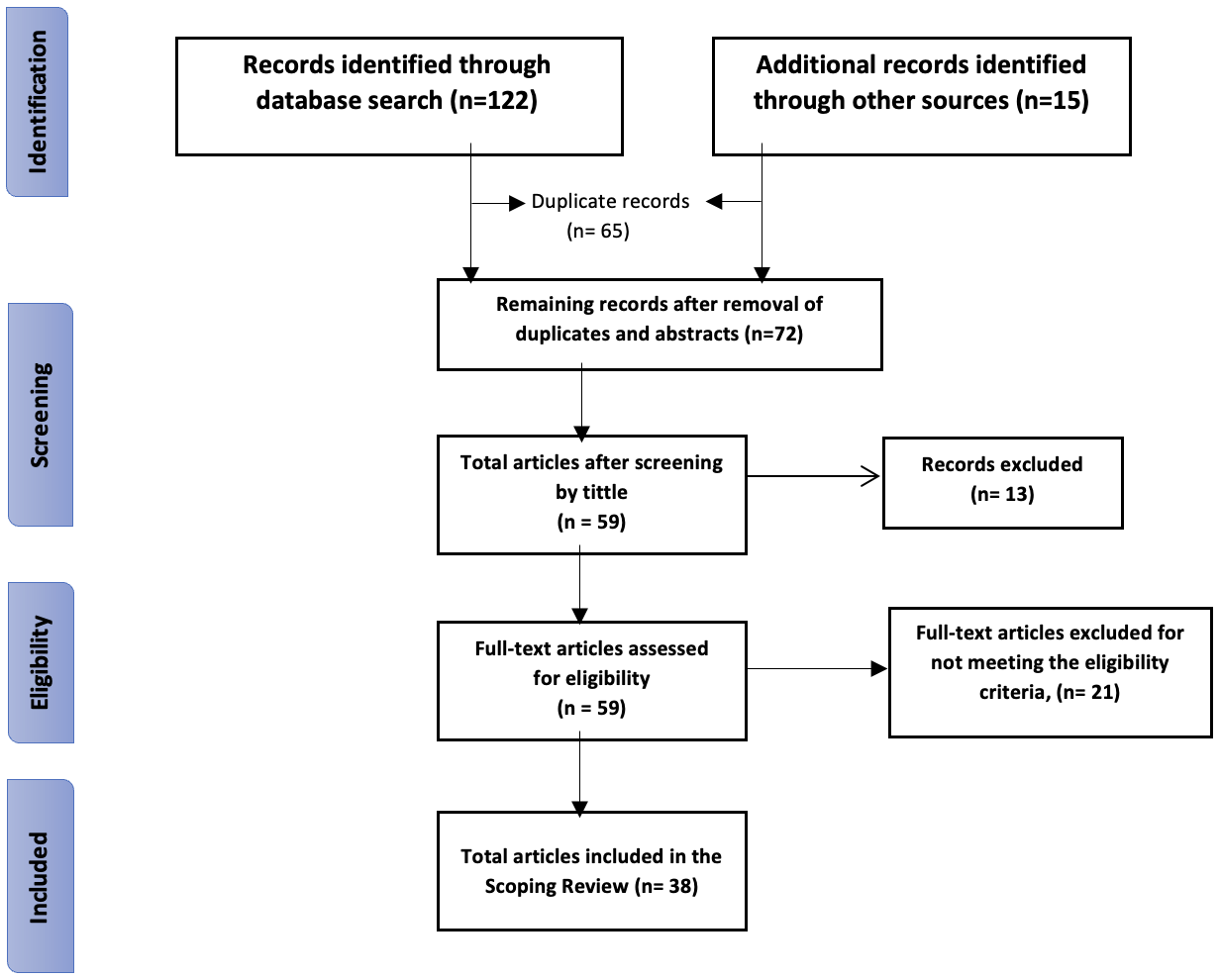
The article screening and selection was done using Microsoft® Excel® for Microsoft 365 MSO (Version 2501 and Endnote 21®. The process was guided by the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement that consists of a minimum set of items guiding the reporting of systematic reviews and meta-analyses9 as shown in Figure 1.
_flow_diagram_s.png)
The PRISMA flow diagram of the article selection process was complemented by the 6-item QATSO to yield eligible articles of high-quality standard as shown in Table 1. At the eligibility stage of the article selection process shown in the PRISMA flow diagram, eligible articles were assessed for quality guided by a validated and adapted 6-item quality assessment tool for systematic reviews of observational studies (QATSO).10 The six-item criteria for determining article quality was composed of six questions that must be addressed, which were: (1) was the sampling method used representative of the study population? (2) was the study sample size statistically determined, or did the study sample size give the study an adequate power? (3) were the eligibility criteria for participants selection clearly stated? (4) were the outcome measures objectively ascertained? (5) were the study outcome measures clearly assessed/determined? (6) were any strategies employed to control for potential confounding/bias, for instance through randomization, stratification, restriction, use of controls, or matching, statistical control, at any of the study design or data analysis stages?.10 Each of the six questions could be answered by a “Yes” or a “No”, where a “Yes” was given a score of 1 point and a “No” a score of 0 points, giving a minimum possible total score of 0 points and a maximum possible total score of 6 points, as shown in Table 1. All the study articles rated as poor were excluded from the final review analysis.
Following the application of the PRISMA statement and the QATSO in article selection, a total of 38 articles were selected for the final review analysis.
RESULTS
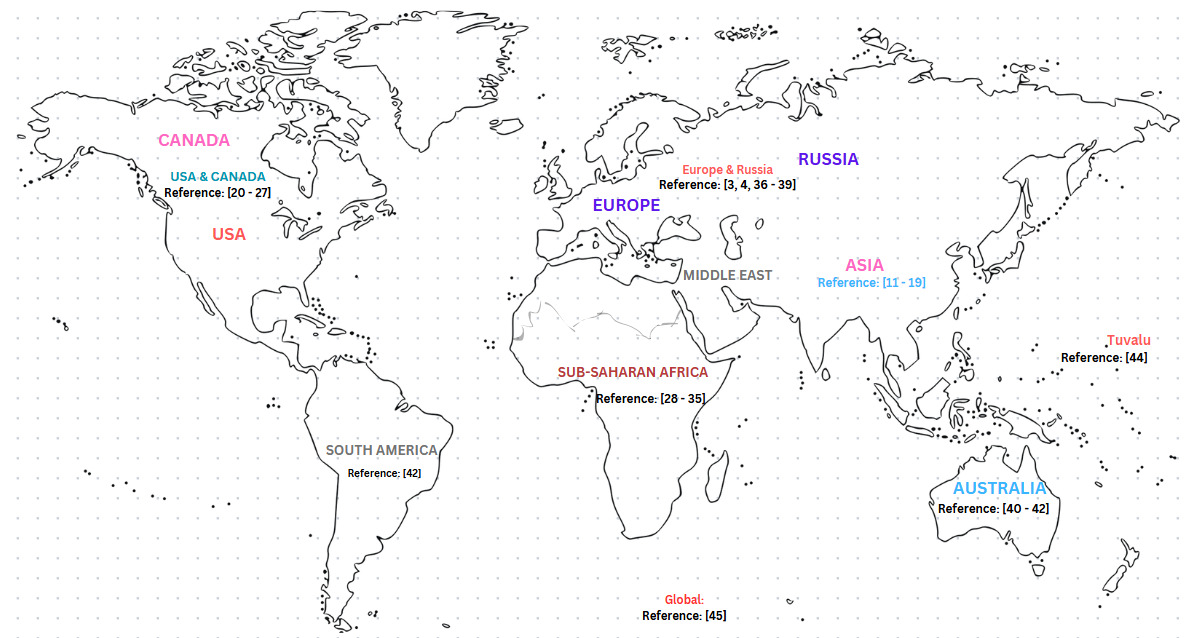
A total of 38 articles were analysed. Most of the articles (over 75%) focused on the effects of heat on human health, as shown in Table 2. The remaining articles were on the effects of drought, or excessive rainfall/floods on human health, with others on the combined health effects of heat, excessive rainfall/floods and drought. Higher numbers of the included articles were from Asia, North America, sub-Saharan Africa and Europe, as shown in Figure 2. The number of publications reporting the health effects of the EWEs under study showed an increasing trend over time, starting from 2015 up to the time of data collection (February 2025). Only one of the included studies evaluated the effectiveness of mitigation measures to EWEs using a quasi-experimental study design.11 There was limited research evidence on implementation science reporting the effectiveness of countermeasures or adaptation innovations against EWEs, and data surveillance information on climate-sensitive diseases/conditions, particularly in low-income countries (LICs).
.png)
Effects of heatwaves, excessive rainfall/floods and drought on human health
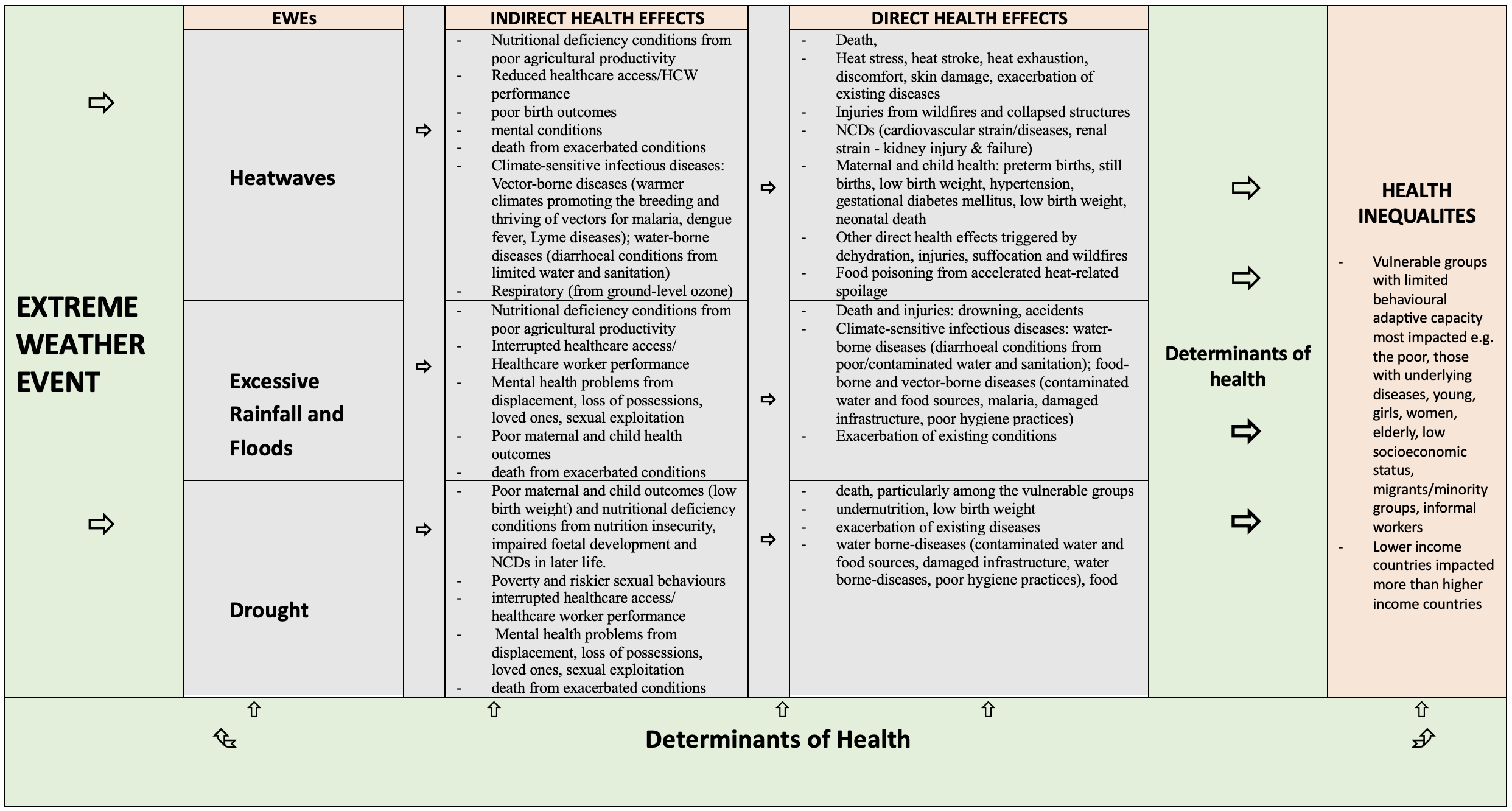
The direct and indirect health effects of heatwaves, excessive rainfall/floods and drought are categorised and summarised in Table 3.

Death, injuries, heat stress, heat stroke, maternal and child conditions consistently emerged as direct health effects of heatwaves.23,24,36,40 Also frequently mentioned were other health effects that are triggered by exposure to excessive heat such as dehydration, wildfires, suffocation, injuries, and food poisoning from accelerated heat-related spoilage. The reported deaths were usually as a result from failure of the body to cope with extreme heat (continued and uncontrolled dehydration leading to kidney/organ failure and death), suffocation or fatal injuries from collapsed infrastructure or wildfires and exacerbated underlying/existing diseases/conditions.2,3,5,13,44
The consistently identified indirect effects from heatwaves on human health were:
-
death from exacerbated conditions caused by heatwave.19,20,22
-
poor birth outcomes from interrupted access to healthcare,
-
poor maternal outcomes such as premature birth, miscarriages and death
-
compromised child nutrition from inadequate maternal nutrition due to reduced agricultural productivity24,35,40
-
exacerbated or emergent mental health conditions23,31,40
-
nutritional deficiency conditions from nutrition insecurity and reduced agricultural productivity caused by excessive heat or excessive rainfalls/flooding fallowing warmer climates,13,28,29,31,35
-
reduced healthcare access/reduced healthcare worker performance5
-
mental health conditions emanating from displacement, uncertainty,19,21,24,35,40 loss of property or loved ones,5
-
vector-borne diseases from breeding and thriving of vectors promoted by warner climates, such as malaria, dengue fever, Lyme diseases,3,14,16,17,33,38,39,42,45
-
diarrhoeal diseases from poor water and sanitation due to water scarcity or diminished water sources.3,14,17,25,39
Consistently emerging direct health effects of excessive rainfall and floods were:
-
death and injuries mainly from drowning, collapsed infrastructure and water-borne diseases,11,12,24,40
-
water-borne diseases such as gastrointestinal diseases - cholera and typhoid from contaminated food and water sources, poor hygiene/sanitation practices,3,14,33
-
vector-borne diseases such as malaria, dengue, yellow fever due to more stagnant water sources promoting vector breeding3,14,16,17
-
exacerbation of existing conditions.5
With regards to the indirect health effects of excessive rainfall and floods, the commonly identified literature findings were death from exacerbated conditions, nutritional deficiency conditions from poor agricultural productivity, interrupted healthcare access or healthcare worker performance, mental health problems from displacement, loss of possessions, loved ones and sexual exploitation/abuse, and poor maternal and child health outcomes due to the interaction of direct and indirect effects.4,33,38,40,42,43
Concerning the direct effects of drought on human health, there was a convergence of findings in reviewed articles consistently reporting death from starvation among the vulnerable groups, undernutrition, poor birth outcomes (such as low birth weight), exacerbation of existing diseases, and diarrhoeal diseases (from poor water and sanitation due to water scarcity and poor hygiene practices).13,29–33,35,44
The indirect health effects of drought that consistently emerged from the reviewed literature include:
-
poor maternal and child outcomes such as low birth weight and miscarriages20,23,27,29,31,36
-
poverty and riskier sexual behaviours due to loss of livelihoods,5,31,32
-
interrupted healthcare access/healthcare worker performance,
-
mental health problems5,32,44 from displacement, loss of possessions, loved ones, sexual exploitation/abuse)
-
death from exacerbated conditions.
According to the foetal origins of adult diseases theory by David Baker, poor nutrition during pregnancy can lead to poor foetal development and low birth weight, and programs the foetus for onset of noncommunicable chronic diseases (NCCDs) in later life.46
EXTREME WEATHER EVENTS, ECONOMIC STATUS AND HEALTH
The articles reported several direct and indirect effects of EWEs on human health as summarised in Table 3. No major variation was observed on the types of health effects posed by each EWE across study locations and over time. It is important to note that the three EWEs under study are inextricably linked together in that the occurrence of one is influenced by the other. For instance, heatwaves can contribute to drought and crop failure, or to floods/excessive rainfall as promoted by warmer climates,5,38,40 and droughts are linked to the formation of hydrophobic soils that in turn promote floods following excessive rainfall.24 This interlinkage can aggravate the magnitude of the impact of these EWEs on human health resulting in increased burden.
It became apparent that there is differential effect of EWEs on human health based on sociodemographic differences – differences in the power and control that people have over societal resources and their lives. At individual level, the power and control emanate from factors such as one’s age, level of education, economic position, employment status, income level, gender, health status, geographic location, ethnicity, race, among others, while at societal level, the power is determined by factors such as political stability and macroeconomic factors, among others.5 These individual and societal factors are collectively called the social determinants of health, for they are the social factors that determine one’s power/advantage to control the resources that are needed to lead healthier lifestyles.5,47 For instance, higher levels of education can be linked to chances for better income and higher social position that can enable one to afford and choose a safer and healthier lifestyle, than those with lower levels of education, lower income, lower social position and with limiting conditions, who are socially deprived and therefore less likely to afford/sustain a safer and healthier lifestyle. Vulnerability to EWEs was shown to vary based on these social determinants of health, where the poorer who are already prone to poor health by virtue of their social deprivation, are also more fragile to EWEs and their effects due to their limited behavioural adaptive capability emanating from having inadequate resources. EWEs can thus exacerbate health inequalities between and within countries, where the poorer are more fragile and bear the greater disease burden.
Effects of HEATWAVES, EXCESSIVE RAINFALL/FLOODS and drought on health inequalities
The articles reported marked inequalities in health outcomes within and between countries.1–5,10–15,17–31,33–45
Lower income countries emerged to be experiencing worst health consequences than higher income countries, particularly due to limited financial resources for adequate preparedness, mitigation and response interventions.5,15,33,40,45 Within countries, the vulnerable population groups, commonly associated limited behavioural adaptive capacity, bear the worst health consequences, namely the poor/people of low socioeconomic status, the elderly, children, women and girls, informal workers, refugees/internally displaced people/migrants and those with underlying diseases/conditions.3,5,32,44
DISCUSSION
The main review findings were that heatwaves, excessive rainfall/floods and drought:
-
pose direct and indirect effects of increasing concern on human health. The main effects include death; injuries and exacerbation of existing diseases/conditions; nutritional deficiency conditions; poor maternal and child health outcomes; mental health conditions; water-borne and food-borne diseases, respiratory and skin conditions; vector-borne diseases; and sexually transmitted diseases. These climate-sensitive diseases/conditions and their determinants are inextricably linked together as are the EWEs themselves.
-
impact differently on human health, within and between countries. The lower income countries and lower socioeconomic population groups are more fragile and experience more vulnerability due to inadequate resources for preparedness, mitigation and response.
-
are still poorly documented – data surveillance and reporting for climate-sensitive diseases is still evolving, particularly in lower income countries.
-
are more discussed about and documented than are acted upon, particularly in LMICs, thereby implying prolonged vain discussions and inaction. Empirical evidence reporting response measures for addressing the health effects of the EWEs, strengthening resilience capacity and enhancing effectiveness of adaptation measures is scant across LMICs. There is generally limited documented information about cost-effective policies, solutions or interventions that utilise locally available resources to address the reported EWEs and their effects, including the exacerbated health inequalities.
Findings from the analysed articles were more complementary than they were replicative or contradictory. This is so, despite the evolving nature of the research topic over time, and the harmonised but diverse study issues, that is, extreme heat, excessive rainfall/floods, drought, climate-sensitive diseases/conditions, and health inequalities. A pattern was apparent where the type and number of reported health effects increased over time (from the early 2000s to February 2025), probably as more interest amassed on the confluence between the increasingly occurring EWEs and health, and as more scientific studies were conducted and published.3,5
The general trend observed from existing evidence is that whereas studies conducted in HICs have reported the health effects of the targeted EWEs and the interventions being implemented to address the challenges, LMICs have mainly reported the health effects alone, with limited to no accompanying climate-sensitive disease surveillance data and addressive interventions.
The agenda of EWEs and human health can be regarded as already bloated with evidence on the health effects and its pertinency, yet generally still deficient of feedback data on existing interventions/countermeasures and on climate-sensitive disease surveillance information, particularly in LMICs.2–5,38,44,47
Recommendations
Given the overwhelming scientific consensus that the effects of EWEs pose a serious threat to human health and health equality2,3,5,38,41,44–48; the paradigm must shift more towards research and implementation science or the generation of practical and contextually relevant evidence-based solutions than continued theory and postulations, particularly in LMI settings.
Such a paradigm shift may involve consideration to test and adapt lessons learnt from high-income or climate change-resilient countries, or measures such as:
-
design and implementation of public policy options that favour technological and behavioural adaptive capability, for example installation of vegetated roofs, afforestation and re-afforestation to protect and restore carbon sinks. This strongly depends on strong political commitment and involvement.
-
investing in policy implementation, research, development and innovation aimed at contributing to climate change resilience. This will ensure public safety/wellbeing by cushioning them from the effects of EWEs, using locally available, appropriate, affordable and sustainable resources and technologies.
-
promoting community literacy on EWEs. This may include dissemination of behavioural-data-informed and community co-constructed information, educational and communication materials on early warning signs for EWEs and recommended preventive/protective/treatment behaviours - e.g. Heat-health warning systems.3,5 This can be more effectively implemented using culturally appropriate, affordable and locally accessible technologies. The vulnerability reduction measures must deliberately target the most vulnerable groups (such as outdoor workers, women, children, girls and disabled people) to address EWEs-attributable social and health inequalities, particularly in LMICs where the majority are outdoor workers due to the expanding informal sector.5,44,48–50
-
promoting research and implementation science on adaptation strategies to EWEs and their effectiveness.
-
integration of extreme weather-related health events into routine care and surveillance system (climate-sensitive diseases surveillance), as a practical public health policy option, given the sparsely available data.
-
strengthening the link between health system resilience and national/global policy frameworks by policy actors, such as the Sustainable Development Goals 3 and 13 and the Sendai Framework for Disaster Risk Reduction (2015 – 2030).3,5,45,47
Study limitations
-
Relevant articles published in languages other than English may have been missed, since the search outputs for this review were limited to those written in the English language. This language barrier may have negatively affected generalizations made in this review.
-
Information contained in offline grey literature or country specific reports may have been missed due to limited access.
-
Publication bias cannot be ruled out. Selective publication based on research results may have led to relevant study findings that could not be published being missed by this study.
-
The heterogeneity of study designs and assessed health indicators from the included studies may imply differential measurement or ascertainment of EWEs and health indicators. Therefore, there is a possibility that similar findings from across the included articles may not have been comparably matched.
-
Due to the scoping nature of the study, the study lacked the merits of quantitative meta-analysis.
CONCLUSIONS
Existing evidence on the health effects of excessive rainfall/floods, heatwaves and drought can be considered an abundant capital to leverage resilience-building/-strengthening interventions, as a matter deserving urgent attention. Considering the alarming global warming trends global, regional and national policy actors must seriously consider utilizing existing climate change evidence to urgently implement appropriate countermeasures. LMICs can adapt lessons learnt from climate-resilient economies and invest in building/strengthening resilience using tested and proven community co-constructed approaches and technologies to protect the public from the health and social effects of EWEs, and to evaluate adaptation strategies.
Ethics statement
This review did not involve human participants and hence did not require ethical approval.
Data availability
The data and materials supporting the results or analyses of this paper will be made available from the corresponding author, Dr. Laston Gonah, Email: lgonah@wsu.ac.za on reasonable request to bona fide researchers.
Funding
No funding was received for the study, either for the sources of evidence or for conducting the scoping review.
Authorship contributions
Gonah L: Conceptualization; Investigation; Methodology; Formal Analysis; Resources; Software, Supervision; Visualization; Writing – original draft; Writing – review and editing. Mabunda S A: Methodology; Validation; Writing – Review and Editing. Faleni M: Methodology; Validation; Writing – Review and Editing. Nomatshila S C: Methodology; Validation; Writing – Review and Editing.
Disclosure of interest
The authors completed the ICMJE Disclosure of Interest Form (available upon request from the corresponding author) and disclose no relevant interests.
Correspondence to:
Laston Gonah
Department of Public Health, Faculty of Medicine and Health Sciences, Walter Sisulu University,
Mthatha 5100, Eastern Cape,
South Africa
lgonah@wsu.ac.za; lggonah@gmail.com