Urogenital fistulas may occur between any part of the genital tract (uterus, cervix, vagina) and nearby organs in the pelvis, including the urinary tract (ureter, bladder, urethra) and intestinal tract (colon, rectum, anus).1 Fistula aetiology is usually clear. Most fistulas occurring in low- and middle-income countries are ischaemic, caused by pressure necrosis when women in prolonged, obstructed labour are not able to have emergency caesarean sections in time to avoid injury to mother and child.2,3 But an increasing number of fistulas are iatrogenic, arising as surgical accidents.4 More rarely fistulas occur from trauma (including sexual violence), radiation, malignancy, unsafe abortion, infection, or as congenital malformation.5 Understanding fistula causes is particularly important as overall access to emergency obstetric care improves, since surgical accidents point to opportunities to improve the quality of care.
Fistulas occurring after prolonged, obstructed labour and vaginal birth, most commonly with a stillborn child, are ischaemic, due to pressure necrosis. Although there are exceptions, it is reasonable to expect that fistulas occurring after gynaecological surgeries are iatrogenic. Aetiology may be less clear when fistula occurs in women who have laboured for a long time before a caesarean birth. In these situations, fistula surgeons might differ in their assessments of fistula cause. Such differences create challenges assessing the epidemiological transition from ischaemic to iatrogenic predominance in fistula surgical caseloads. Together with limited survey data and methodological challenges, the lack of consensus on iatrogenic fistula definitions contributes to the reality that population-level incidence and prevalence of iatrogenic fistula are unknown. Measurement with shared definitions can encourage appropriate actions to address iatrogenic fistula occurrence.
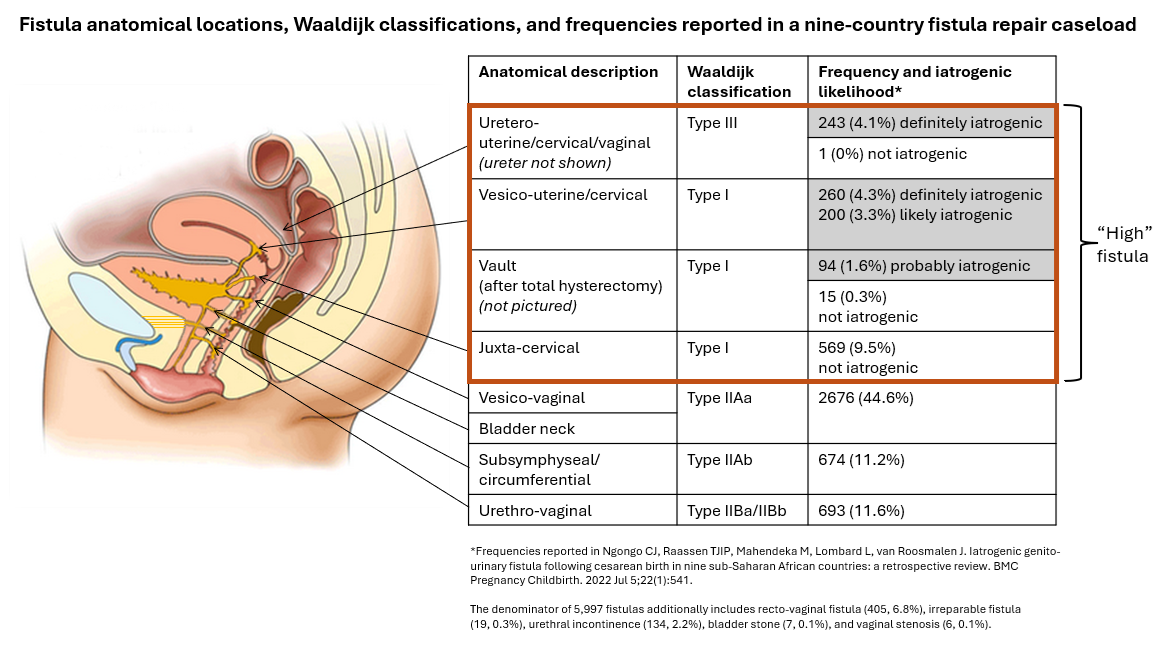
Three of us (TJIPR, CJN, and MM) proposed a conceptual categorization for understanding the likelihood of iatrogenic origin based on anatomical location and circumstances, based on TJIPR and MM’s decades of experience repairing fistulas.4 Figure 1 describes the anatomical locations of 5,997 previously reported fistulas, together with their likelihood of iatrogenic origin.6 “Definitely iatrogenic” fistulas occur away from where foetal head pressure against the mother’s pelvis would lead to ischemia and necrosis. “Probably iatrogenic” and “likely iatrogenic” categories recognize increasing ambiguity. The categorization takes into account whether the baby was alive or stillborn in cases of caesarean section following prolonged, obstructed labour. We applied this conceptual categorization to report that 13.2% (788/5,959) of repaired fistulas were iatrogenic, including 26.8% (787/2,942) of women with fistula following caesarean birth.4,6 Caesarean section can be complicated in women who arrive late to facilities with prolonged, obstructed labour and in women with scarring from previous abdominal or pelvic surgeries, increasing the risk of iatrogenic fistula. Fistula aetiology may not matter substantially in treatment decisions for individual women, although surgical outcome data suggest higher repair success for iatrogenic fistulas than ischaemic fistulas.

Reports from Ethiopia and Malawi have used the broad and less-specified category of “high bladder fistula” occurring predominantly after surgery, which constituted approximately one-quarter of urinary fistulas repaired (24.6% (638/2,593) in Ethiopia and 26.3% (119/452) in Malawi).7,8 This approach focuses on fistula location, contrasting “high” fistulas (into the vaginal vault, cervix, or above) with ischaemic “low” fistulas below this level. The category of “high” fistulas includes “juxtacervical, intracervical, uterovesical [vesico-uterine], vault fistula, and ureteric fistula.”7 While this grouping broadly overlaps with the iatrogenic fistula categories we have previously proposed, it might include fistulas that may not be iatrogenic, despite their location, such as juxtacervical fistulas. While most “high” fistulas will be iatrogenic, it is unlikely that they all are.
The term “high” seems to be a nonspecific term subject to diverse interpretations. Presumably “high” is meant in an anatomical sense connected with genital tract organs, rather than a standard distance from any fixed point, which is important given anatomical diversity. Yet the term invites confusion between the cervix (which is usually high, except in cases of prolapse) and fistulas high in the vagina. Defining ureteric fistulas as “high” may erroneously suggest that ureteric injuries are high in the ureter, even though ureters are most frequently injured near their entrance into the bladder. We urge fistula surgeons to use clear anatomical terms when summarising likely fistula causes to enable comparisons over time and across contexts.
It appears that an iatrogenic aetiology of obstetric urogenital fistula is a growing problem irrespective of definitions.6,7,9 Iatrogenic fistula constitutes a rising proportion of the fistula caseload in Africa and South Asia, particularly as women gain access to emergency obstetric care. Some of us previously reported that the odds of iatrogenic origin nearly doubled between 1994-2017 among fistulas repaired in nine African countries (adjusted odds ratio=1.94, 95% confidence interval 1.48-2.54).6 Escalating hysterectomy rates may also increase opportunities for accidents. The risk is particularly acute in remote locations where health providers do the best they can despite difficult caseloads and insufficient resources, including, in some cases, surgical expertise.10
Bladder and ureteric injuries will continue to happen as long as surgeons operate on patients. Fistula surgeons play an important role in identifying iatrogenic fistula occurrence. Healthcare providers, managers, and policymakers can prevent many iatrogenic fistulas through ensuring appropriate work environments, clear safety standards, accountability mechanisms, and robust provider training. Although sometimes limited by incentives and time availability, healthcare provider mentorship and regular feedback on technique, genuine indications for surgery, and case selection can additionally promote high-quality patient care.
Universal and consistently employed definitions for iatrogenic fistula facilitate common solutions and enable comparisons in population-level fistula causes over time and across geographies. Such epidemiological analysis constitutes a core objective of global health practice and can inform prioritization and funding decisions. Achieving clarity and agreement on iatrogenic fistula definitions may require policymakers and practitioners to extrapolate successful strategies that have been used to implement change in other areas. Facilitated discussion may help fistula surgeons to reach consensus. Tracking fistula causes over time can inform targeted quality improvement approaches and promote accountability for providing the best possible quality of care for women.
Acknowledgements
We thank the International Federation of Gynecology and Obstetrics (FIGO) for supporting online open access.
Funding
This viewpoint was developed without support from external funding. The article publication charge was funded by FIGO.
Authorship contributions
CJN, TJIPR, and PH led the conceptualization and writing of the original draft. MM, SA, and LW reviewed and edited the draft.
Disclosure of interest
The authors completed the ICMJE Disclosure of Interest Form (available upon request from the corresponding author) and disclose no relevant interests.
Correspondence to:
Carrie Ngongo
RTI International
3040 E Cornwallis Road
Research Triangle Park, NC 27709
USA
cngongo@rti.org
cngongo@gmail.com