INTRODUCTION
The COVID-19 outbreak, declared on the 30th January 2020 by the World Health Organisation (WHO) as a public health emergency of international concern affected all the continents and about 228 countries in the world.1 As of the 23rd of February 2023, there were 757,264,511 confirmed cases in the world and 6,850,594 deaths.2 Cameroon was not spared and registered its first case on the 6th of March 2020.3 By February 26, 2023, the Cameroon Public Health Emergency Operation Coordination Centre (PHEOCC) declared 125,011 cases and 1,972 deaths.4 The two most affected regions were the Centre region and the Littoral region with 38,594 cases and 522 deaths, and 35,573 cases and 389 deaths respectively.5
The pandemic caused a significant disruption in the healthcare system, impacting the availability and utilisation of health services. The United Nations Children’s Fund (UNICEF) and WHO estimated that about 23 million children missed their routine vaccination in 2020 which is 3.7 million more than in 2019.6 Early into the pandemic in Brazil, Pakistan, and Afghanistan, COVID-19 harmed routine vaccination.7–9 Worldwide, with various measures implemented to address the pandemic, there was a notable decrease in paediatric hospital visits and the use of services, particularly for routine childhood vaccinations10 and Cameroon was no different. Based on the hypothesis that the COVID-19 pandemic and the associated countermeasures led to a decline in vaccination activities and coverage at the regional level, we aimed to quantify the pandemic’s impact on the Expanded Program of Immunisation in a severely affected region of Cameroon and compare this effect between rural and urban districts within this region.
METHODS
Study design, setting and sampling
A descriptive and analytical cross-sectional observational study was conducted, using secondary data from the District Health Information System-2 (DHIS-2) of Cameroon, the COVID-19 situational report provided by the Public Health Emergency Operation Centre (PHEOC), and data on containment measures obtained from an international online data platform (https://ourworldindata.org/coronavirus).
The Littoral region is one of the Coastal regions of Cameroon and lies between the South region, the West region, the Centre region and the Southwest region. In 2021, its population was estimated at 4085142 representing about 16% of the total countries’ population. It has 4 administrative divisions consisting of 24 health districts divided into 9 urban districts and 15 rural districts. It has a population density of 188.8 and has about 2.96 Health facilities per 10000 inhabitants.11 It was purposively chosen, as it represents, according to PHEOC, the second most affected region in Cameroon, accounting for 28.5% of the total number of cases registered.12
The Expanded Program of Immunisation was chosen as a proxy to service utilisation and demand because it is offered by more than 60% of registered health facilities (both private and public at all levels of the health pyramid) in Cameroon.13 The 4 chosen vaccinations are given at other time points in the first year of life of a newborn: BCG vaccination represents the initial encounter with the vaccination service, and as it is given at birth, it gives an indication of the use of health services for deliveries; PENTA1 (given at 6 weeks) and PENTA3 (given at 10 weeks) were identified as relevant indicators in adherence to the Cameroon Ministry of Health’s criteria for measuring vaccination access. For measles vaccination (administered at 9 months), mothers need to come explicitly for this vaccination to the health service and is, hence, a good proxy for service utilisation.
Data collection and storage
The percentage of children vaccinated versus those expected for BCG, PENTA1, PENTA3, and Measles vaccines for the two years preceding the first recorded COVID-19 case (Pre-COVID), as well as the two years following the onset of the pandemic in March 2020 (COVID) were extracted. However, given that the reporting rates for hospitals and health centres in the Littoral region were 59.5% and 48.8%, respectively, in 2018,14 data from 2018 were excluded from the analysis. This is because the completeness of less than 70% is said to alter the exactitude of data generated. Both monthly and yearly coverages were available at the regional level, while only yearly data were available for the 24 districts. The number of COVID-19 cases for the Littoral region was extracted from the situational reports (SITREP) of the PHEOC. These reports were issued weekly, and a simple method of addition and subtraction was employed to derive monthly data. The stringency index (developed at Oxford University to track government policy responses by calculating a daily mean score based on nine metrics: school closures, workplace closures, public event cancellations, restrictions on gatherings, public transport closures, stay-at-home orders, public information campaigns, internal movement restrictions, and international travel controls with each metric being scored between 0 and 100) was obtained for Cameroon as a country from the website https://ourworldindata.org/coronavirus. To establish a monthly index, the highest stringency index recorded within each month was considered.
The two data set used are presented in Table S1 and Table S2 in the Online Supplementary Document.
Data analyses
The various datasets were collected and compiled in an Excel spreadsheet. Then, data were exported directly to R-studio software or converted to CSV files for compatibility with the Quantum Geographical Information System (QGIS).
We had 2 main data sets. The first one was the monthly Littoral vaccination coverage together with the monthly COVID-19 cases and monthly COVID-19 stringency index (Table S1). It was used for visualisation of tendencies and analysis of the impact of COVID-19. The second data set was composed of the yearly vaccination coverages per district to assess the differential impact of COVID-19 on rural versus urban districts (Table S2). Time series analysis was performed and plotted with regards to the Pre-COVID period (January 2019-February 2020) and COVID period (March 2020-December 2021).
Analysis of associations was done using simple linear regression when the dependent variable was numerical, or bivariate analysis to obtain a correlation coefficient or non-parametric Wilcoxon rank sum test to ascertain if the declines observed were significant or not. RStudio (Version 2022.07.2 + 576) and QGIS (version 3.22) were used.
To ascertain correlation, a weak association was between 0.5 and 0, a moderate association between 0.6 and 0.7 and a strong association above 0.8 to 1.
Ethical Considerations
This study did not involve any individual-level data, so ethical clearance was not required. However, being conscious of the fact that the data used (vaccination coverage) belongs to the Cameroon Government, permission to use the data was sought and given by the Director of the EPI programme and the Regional Delegate of Public Health in the Littoral region. To ensure the integrity of the research findings, we eliminated the year with a completion rate of less than 70% to address the inaccuracy of the data.
RESULTS
For this analysis, we defined the ‘Pre-COVID period’ as the entire year of 2019 and the first two months of 2020, before the first reported COVID-19 case in Cameroon. Specifically, this time frame spans from January 2019 to February 2020. The ‘COVID period,’ on the other hand, refers to the duration from March 2020 to December 2021.
Cameroon’s Littoral region is composed of 24 health districts. Of these, 15 districts are classified as rural, including Abo, Dibombari, Edea, Loum, Manjo, Manoka, Mbanga, Melong, Ndom, Ngambe, Njombe Penja, Nkondjock, Nkongsamba, Pouma, and Yabassi. The remaining districts Bangue, Boko, Bonassama, Cité des Palmiers, Deido, Japoma, Logbaba, New Bell, and Nylon are urban.
Spatial and temporal distribution of EPI coverages
The data indicates a significant decline in vaccination coverage during the COVID period, particularly for PENTA1 and PENTA3 vaccines. Urban districts, which initially had high vaccination rates, saw notable decreases. For instance, in Cité des Palmiers, the PENTA1 vaccination coverage dropped from 101.3% in 2019 to 82.7% in 2021. Similarly, Bonassama’s PENTA3 coverage fell from 92.7% in 2019 to 78.3% in 2021.
The decline was even more pronounced in rural districts. Yabassi, for example, experienced a drastic reduction in PENTA3 coverage, from 77.9% in 2019 to 48.7% in 2021. Pouma also saw a significant decrease in PENTA1 coverage, dropping from 100.3% in 2019 to 60% in 2021 (as detailed in Table S3).
While the declines in PENTA1 and PENTA3 were substantial, BCG vaccination coverage showed a different trend. In some districts, BCG coverage even increased during the pandemic. For example, in the urban district of Bangue, BCG coverage rose from 82.6% in 2019 to 90% in 2021. Conversely, Manjo experienced a slight decrease in BCG coverage, from 59.7% in 2019 to 55.8% in 2021 (Table S3).
However, measles vaccination coverage dropped significantly in both rural and urban districts during the COVID period. In Abo, a rural district, measles vaccination coverage plummeted from 114.6% in 2019 to 72.9% in 2021. Similarly, the urban district of Deido saw its measles vaccination coverage fall from 83.8% in 2019 to 56.7% in 2021 (Table S3).
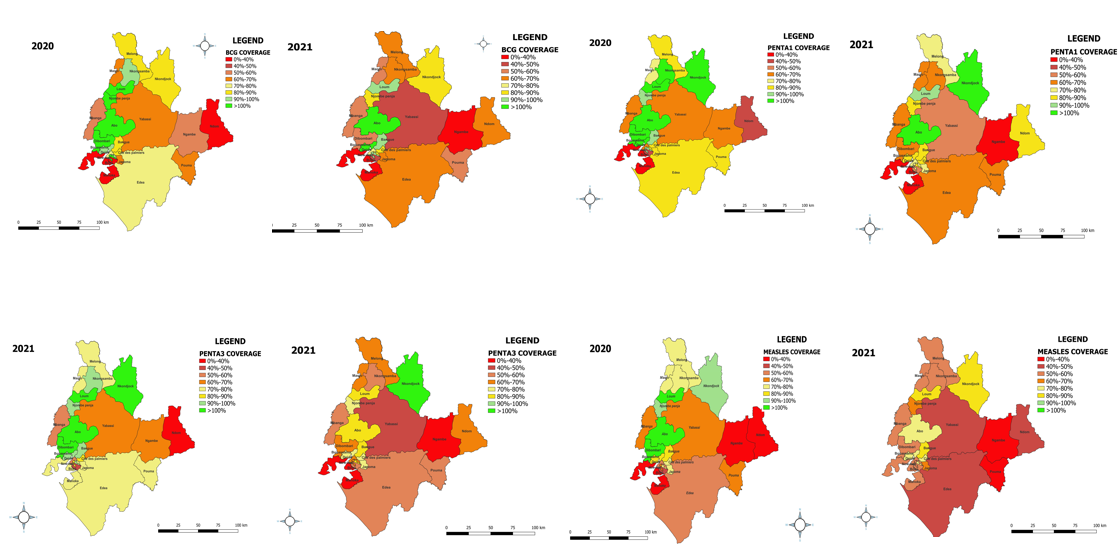
Though 2 years into the pandemic, vaccination coverages dropped, following the declaration of COVID-19 in Cameroon in March 2020, there was an overall increase in BCG and Measles vaccination coverages by about 10% and then a gradual drop from June 2020 to reach the lowest coverages (60%) early in 2021. Contrary to what is seen in the BCG coverages, PENTA1 showed a transient drop following the declaration of the pandemic, rose transiently till June 2020 and subsequently dropped to reach the lowest coverage early in 2021. PENTA3 coverage was quite different and showed a different trend as it dropped following the declaration, rose briefly at the start of 2021 then reduced to reach the lowest coverage in the second half of that same year. Hence, though globally we see a drop in coverage through the years 2020 and 2021, the drops are proportional to each district. Districts with poor coverage tend to worsen vaccine coverage over time and districts with good coverage tend to maintain the coverage as shown in Figure 1.

The other data are presented in Table S3 in the Online Supplementary Document
Temporal evolution of the COVID-19 pandemic and COVID-19 stringency index in Cameroon
Common to all the coverages and as seen in the temporal distribution, the lowest coverages were found in 2021, about 10 months into the COVID-19 pandemic as shown in Figure 2.
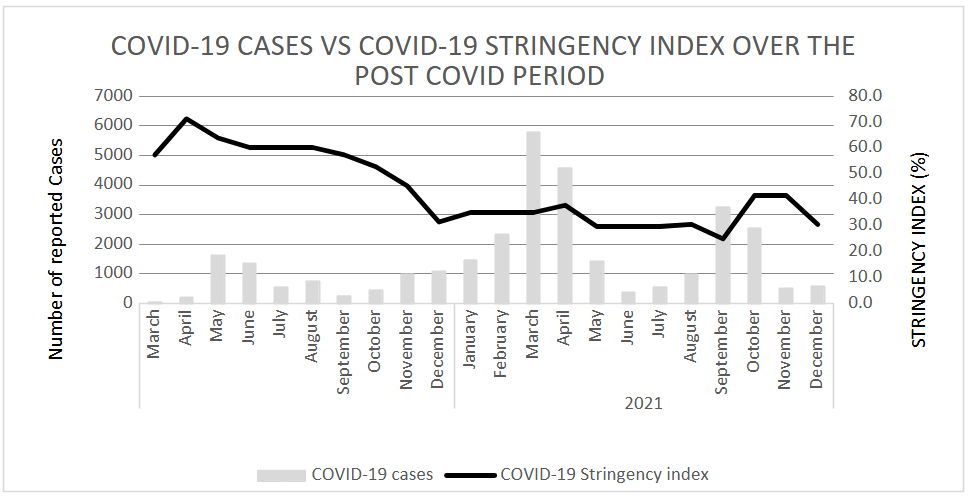
There is no direct link between the COVID-19 cases and the COVID-19 stringency index as seen in Figure 3. During the first wave of the pandemic (May 2020 – August 2020) the stringency index was quite high (above 70%) in contrast with the reported number of cases (highest monthly reported cases 1616). Nevertheless, between January 2021 and May 2021when the second wave was reported, some measures such as schools re-opening had been lightened, resulting in a stringency index of 40% though there was a higher number of reported cases (Highest monthly reported cases 5790).

Association of Vaccination Coverage with COVID-19 Cases and COVID-19 Stringency Index
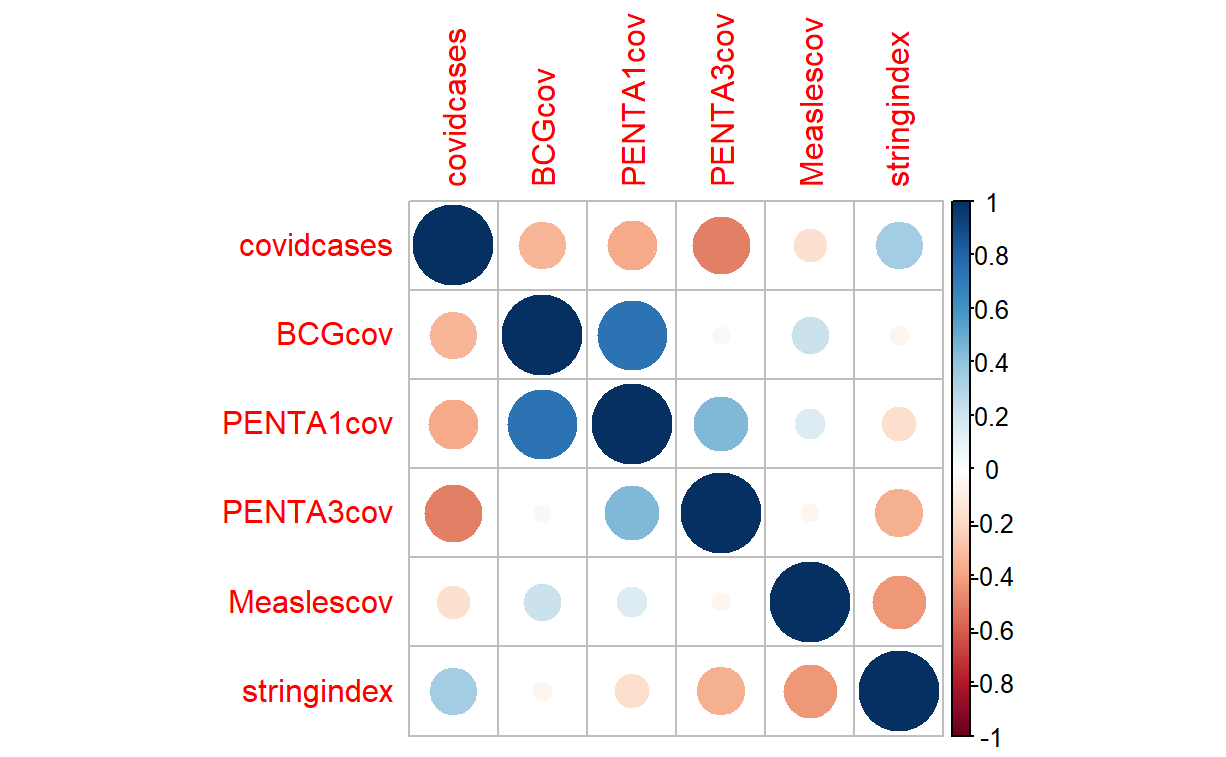
Figure 4 shows the association between COVID-19 cases, COVID-19 stringency index, BCG, PENTA1, PENTA3 and Measles coverages. We observed a positive yet weak correlation between COVID-19 cases and the COVID-19 stringency index with a coefficient of 0.34. Between PENTA1 and BCG, there was a strong positive correlation of 0.73, being 0.45 between PENTA1 and PENTA3. There existed a negative, not-significant correlation between COVID-19 cases and three out of the four different EPI coverages, with correlation coefficients of -0.34, -0.37, and -0.17 for BCG, PENTA1, and Measles, respectively. The associations are within the category of ‘moderate’ for COVID-19 cases and PENTA3 with a coefficient of -0.51. This negative correlation was also not significant between the stringency index and the different coverages (BCG: -0.05; PENTA1: -0.18; PENTA3: -0.35; and Measles: -0.44) as shown in Table 1.

Impact of the COVID-19 Pandemic on EPI Vaccination
In all 4 antigens, we found a drop in coverage and this drop was statistically significant for three of the four selected vaccination coverages (PENTA1, P=0.031; PENTA3, P=0.008 and Measles P=0.002) as shown on Table 2.
When considering the entire COVID period, the estimated drops were significant for PENTA1, P=0.041; PENTA3, P=0.002 and Measles, P=0.001. As for BCG vaccination coverage, the drop observed is not significant. Nevertheless, when considering individual years, while measles coverage has been affected by the COVID-19 pandemic and the related containment measures in both years, BCG coverage has not been significantly affected in either year. PENTA1 and PENTA3 were significantly affected only during the second year following the start of the pandemic as shown in Table 3.
Impact of the COVID-19 Pandemic on Urban versus Rural Districts
Overall, when considering the pre-COVID and COVID periods between the urban and rural districts, there was no significant difference, except a borderline difference for BCG coverage (P=0.049). In 2019, the pre-COVID period, and 2020, the first year of the pandemic, there were no differences in EPI coverage between urban and rural districts. In 2021, we observed that all coverage percentages were dropping more importantly in rural areas, however, the differences were only significant for BCG (P=0.035) as seen in Table 4.
DISCUSSION
The expanded program of Immunisation had a great impact in Cameroon for vaccine-preventable diseases such as Rubella, and Cameroon was declared by WHO15 wild polio-free in June 2020. With the advent of the DHIS-2 in 2018, and better documentation of the EPI coverages, we expected to see a rise over time, but this trend changed due to the COVID-19 pandemic. In this study, we evidenced that, when comparing the period after the start of the pandemic with the Pre-COVID period, there has been a non-significant drop in BCG vaccination coverage of 4.75% (P=0.3) and significant drops of 7.83% (P=0.04), 9.55% (P=0.002) and 12.11% (P=0.001) in PENTA1, PENTA3 and Measles coverage respectively in the Littoral region of Cameroon. These results are similar to a study which assessed the effect of COVID-19 in the two most affected regions of Cameroon.16 The results are also in line with several studies in sub-Saharan Africa and the world.17–21 Nevertheless, when comparing our findings with other studies, it should be noted that our findings show rising vaccination coverage at the very start of the pandemic contrasting therefore the other studies where the impact was felt at the very beginning of the pandemic. Moreover, our study demonstrates there was no association between the EPI vaccination coverage and COVID-19 case numbers as seen in Table 1 which in most studies turns to be deductive.17–21 Rare studies showed the opposite of our findings, namely the ones carried out in Kenya and DRC where vaccination coverage either did not change significantly or increased after the start of the pandemic. This difference can be explained by the fact that while in DRC,22 they used data from 3 local health centres where due to lockdowns individuals preferred vaccinating the children locally, our study is a regional data capturing vaccination coverages at all localities and all levels of the pyramid. Whereas in Kenya, the inclusion criteria for the retrospective study included all children in the community eligible for vaccination (both those who use the routine vaccination services and those who benefitted from catch-up vaccination plans), our study targeted children using the routine services as reported in the different hospitals in the region.23 This may also explain why, though the disruptions existed and the drops were significant in most African countries, catch-up vaccination plans had a great positive impact on the nations’ reports.24
An unanticipated finding which not so many other research concentrated on is the disparities between routine vaccination in rural versus urban zones. Our study identifies that vaccination coverage did not reduce with increasing cases, but reduced more in rural zones than urban zones. In the United States of America as far back as 2017 before COVID-19, they identified that children living in non-metropolitan statistical areas had lower coverage than children in principal metropolitan areas.25 Though these COVID-19-related drops in rural zones were also felt in Sierra Leone, no comparison was made with the urban zones.21
In an attempt to contextualise these results and what they mean for Cameroon, we used two different frameworks (Annexes 3 and 4) that intend to answer how social determinants of health and human behaviour can affect the outcome of an intervention such as vaccination.
Within the first framework (elaborated by WHO), four main mechanisms of impact of the COVID-19 pandemic on routine immunizations can be identified,24 namely routine immunization session disruptions, vaccine supply disruptions, vaccine demand disruptions and health workforce diversion. In our setting in Cameroon, two of these mechanisms could have played a role: Vaccine demand disruptions and health workforce diversion. Concerning the vaccine demand disruption, the risk perception of the population was quite low at the start of the pandemic, but this changed in early 2021 when governmental communication of the pandemic increased and so was the awareness among the population who turned to shy away from hospitals,26 as was also described in India.19 This mechanism may explain the drops observed for PENTA1, PENTA3 and Measles in our study. As for health workforce diversion, in an attempt to adapt containment policies and respond effectively to the pandemic, several health staff from hospitals were diverted to COVID-19 treatment centres and from rural to urban areas.
In literature, little seems to have been published in terms of associating the socioeconomic situation of the populations with the vaccination coverage drop during the COVID-19 pandemic. Nonetheless, in the Littoral region, rural districts characterised by lower socioeconomic conditions were found to experience a greater impact compared to urban districts characterised by higher socioeconomic statuses. Since EPI vaccinations are provided free of charge, this outcome may initially seem improbable. However, considering that over 25% of the population in the country lives below the poverty line,27 with a higher concentration of these individuals residing in rural areas28 where proximity to hospitals is lower,29 we anticipate that indirect costs will play a significant role. This is particularly relevant during the COVID-19 pandemic, when factors such as increased prices of essential items like food and transportation were experienced, exacerbated by lockdown measures that restrict routine commercial activities.
The second framework seeks to answer how the knowledge of the illness, the perceived severity and the perceived susceptibility towards the disease can influence the health-seeking behaviour of an individual. In this study, it was used to discuss and explain why there was an initial rise in the EPI coverage and then a reduction. We hypothesised that knowledge of COVID-19, its perceived severity and susceptibility could have influenced the population’s health-seeking behaviour and hence demand for vaccination at different periods into the pandemic. Moreover, infodemics such as rumours, stigma and conspiracy theories have proven to be effective in developing mistrust in the government and its health structures and reducing health-seeking behaviour.30 This might explain why there was more reluctance to seek vaccination services as the pandemic was evolving.
Strengths and limitations
The main strength of this study is the use of readily existing online data from the DHIS-2 platform with a completeness of 100% both in the Pre-COVID period (since 2019) and the COVID period making the study a reliable one to make significant conclusions on the trends observed. Moreover, the conclusions of this study can be used to inform the research community and the policy-makers on what happened in Cameroon during the COVID-19 pandemic and the recommendations can be used for pandemic preparedness and readiness. Also, the robustness of the methods used makes the conclusions of this study reliable.
Even though the conclusion of this study can be useful in informing policymakers in case of another health shock, it presents some limitations. First, the ones known to the use of secondary data where the quality of the data can be affected during the stages of data collection, data entry and data manipulation into the platform.
Secondly, because of incomplete data before 2019 (DHIS-2 started only in 2018), we could not extend the baseline (Pre-COVID period) and had to limit our study to 1 year before COVID-19 and 2 years after the start of COVID-19 restricting the possibility to assess possible trends that could have been present over previous years.
Thirdly, the stringency index derived from officially declared containment policies may not capture the contextual differences in the country in implementing these policies. However, we do not expect a difference that could substantially bias our results.
Fourthly, we attempted to find the difference in impact between rural and urban zones but within each district, there might exist heterogeneity (e.g. difference in socio-economic status) not captured in this study.
CONCLUSIONS
The COVID-19 pandemic substantially impacted routine vaccination coverage in Cameroon’s Littoral region. While BCG vaccination, given at birth did not decline, significant declines were observed in vaccines such as PENTA1, PENTA3, and measles. While urban districts managed to maintain relatively better vaccination coverage, rural districts experienced more pronounced drops, highlighting disparities likely influenced by socioeconomic factors and health workforce diversion during the pandemic. The findings underscore the critical need for targeted strategies (e.g. mobile clinics, non-diversion but recruitment of health workforce) to sustain immunisation efforts during public health crises, particularly in vulnerable and underserved areas.
RECOMMENDATION
It is recommended that complementary qualitative studies be conducted in Cameroon to investigate the contextual factors (health infrastructure, public behaviour etc.) that contributed to the decrease in EPI vaccination coverage. These studies will also add more in-depth into behavioural and contextual factors involved in the vaccination trends observed and the disparities noticed between the urban and rural districts. Understanding these factors will enable better preparedness for future epidemics and help alleviate strain on the healthcare system.
When putting in place response strategies, rural vulnerabilities should be taken into account and tackled appropriately for example initiating mobile clinics in times of health shocks such as the COVID-19 pandemic.
Acknowledgements
We are grateful to all the contributors to this paper.
Data availability
The data used for this article is publicly available on the District Health Information System-2 (DHIS-2) of Cameroon, the COVID-19 situational report provided by the Public Health Emergency Operation Centre (PHEOC) in Cameroon, and on an international online data platform https://ourworldindata.org/coronavirus. The two data set used are also available in the Online Supplementary Document.
Funding
The research presented in the manuscript was indirectly funded by the Belgian DGD by funding my Master Degree. The article publication charge (APC) was funded by the West African Network of Infectious Diseases ACEs (WANIDA).
Authorship contributions
Conceptualisation: MB, VV, CN,
Drafting of the manuscript: MB, CN
Editing/revision of the manuscript: MB, CN, JD, VV, PKQ, AMM, PT, FB
Approved final version: All Authors
Disclosure of interest
The authors completed the ICMJE Disclosure of Interest Form (available upon request from the corresponding author) and disclose no relevant interests.
Additional material
The article contains additional Online Supplementary Document.
Figure 2: Temporal Distribution of BCG, Measles, PENTA1 and PENTA3 vaccination coverages in the Littoral region, Cameroon, 2019-2021.
Correspondence to:
Binyet epse Mbenoun Binouna Annette Olivia Manfreddy
Medecins Sans Vacances
29 Avenue Basoko, Gombe, Kinshasa
Democratic Republic of Congo
Manfreddy.Binyet@msv.be