INTRODUCTION
Diarrhea remains a significant global public health concern, particularly among children under the age of five, with an alarming 1.7 billion cases reported annually, resulting in approximately 443,832 deaths worldwide.1 Less developed countries bear a disproportionate burden, where children under three years experience an average of three diarrheal episodes in a year.1,2 The recurrent diarrheal episodes are associated with acute morbidity as well as long-term adverse health outcomes such as malnutrition, growth stunting, and compromised neurodevelopment.2 The interconnection between malnutrition and diarrhea has been consistently reported over the years,3 where diarrhea is a leading cause of malnutrition in children under five,1 and malnutrition exacerbates the severity of diarrhea.3,4
The World Health Organization (WHO) defines malnutrition as “deficiencies, excesses, or imbalances in a person’s energy intake and/or nutrients”.5 This encompasses several conditions, including undernutrition (wasting, stunting, underweight, inadequate micronutrients), overweight, and obesity.5 In 2022, an estimated 149 million children under the age of five were identified as stunted, 45 million as wasted, and 37 million as overweight or obese, with nearly half of the related deaths occurring in low- and middle-income countries.5 When malnutrition and diarrhea coexist, the risk of mortality and adverse outcomes significantly increases among children.6
Efforts to address this dual burden have been guided by frameworks like WHO’s integrated Global Action Plan for Pneumonia and Diarrhea (GAPPD) and its recommendations for managing severe acute malnutrition in infants and children. These guidelines recommend a multifaceted approach, including oral rehydration solution, continuous feeding, zinc treatment, and antibiotics for specific strains.7–9 However, while effective, these existing frameworks mainly focus on immediate treatment and do not adequately address the nuanced needs of children with both diarrhea and malnutrition who are at heightened risk of mortality. For these vulnerable children, additional measures of comprehensive care involving follow-up and close monitoring are critical in improving clinical outcomes.10–12
Recognizing that reinfections are common in malnourished children13 and that two-thirds of diarrhea-related deaths occur beyond seven days post-presentation,14 we aimed to highlight the effectiveness of a more comprehensive approach– termed enhanced care– for the management of undernourished children with diarrhea. WHO has not previously issued recommendations related specifically to enhanced care for children aged 0 to 10 years with diarrhea. Therefore, this systematic review, commissioned by WHO, evaluates the effectiveness of enhanced care compared to current standard care in improving clinical outcomes among malnourished children experiencing acute watery or persistent diarrhea and dehydration.
METHODS
Types of studies
We included observational, quasi-randomized experimental, and individual and cluster randomized controlled trials (RCTs) published in English from 1 January 2000 to 30 November 2023. The review excluded case reports, case series, opinions, editorials, conference abstracts, reviews, and systematic reviews. Studies that did not report the clinical outcomes of interest were also excluded.
Types of participants
Studies focusing on malnourished children, including those with stunting, wasting, severe acute malnutrition (SAM), moderate acute malnutrition (MAM), or overnutrition aged 0 months to 10 years, experiencing acute watery or persistent diarrhea with or without dehydration, were included. Diarrhea in this population was recognized as resulting from infectious etiology, triggered by underlying disease (for example, diarrhea in SAM) or iatrogenic (for example, antibiotics given in SAM). Diarrhea due to all three causes was included as it was not possible to identify the exact cause of diarrhea. Both inpatient and outpatient populations were included. Studies conducted in children older than ten years or adults were excluded. Studies in which the control care group did not receive standard care and where the intervention was focused on providing or increasing access to standard care, i.e., ORS, IV hydration, zinc, and capacity building of providers, as well as studies based on prevention such as increasing access to water, sanitation, and hygiene (WASH) facilities were excluded. Animal studies were also excluded. Studies with children suffering from chronic or bloody diarrhea (dysentery) were also excluded.
Types of interventions
Intervention: Enhanced care was defined to include hospitalization, close clinical monitoring, longer follow-up after completion of treatment- community-based or ambulatory follow-ups, any treatment beyond the standard care of oral rehydration and zinc supplementation, or any other intervention defined by the author as enhanced care. Additional treatment for the underlying malnutrition, such as ready-to-use therapeutic foods for SAM, was not considered as enhanced treatment. Studies in which the additional treatment was not the same between the groups were excluded.
Control: Current WHO recommendations for the management of diarrhea.1
Types of outcome measures
Studies that reported one or more of the following outcomes were included:
-
Clinical deterioration/treatment failure (Need of hospitalization, worsening of symptoms or as defined by author)
-
Mortality (up to 30 days)
-
Reinfection (up to 30 days)
-
Serious adverse events (SAEs) as defined by good clinical practices (GCP)15
The definition of enhanced care was finalized through a structured consensus-building exercise with subject experts in the team and WHO. The process included extensive discussions on the social determinants and clinical factors that influence this high-risk population’s care. This consensus-building exercise ensured that the definition was reflective of practices tailored to the target population and thus included critical components such as hospitalization, close clinical monitoring, and extended follow-up after treatment completion- community-based or ambulatory follow-ups, beyond the standard care of oral rehydration and zinc supplementation.
Search methods for identification of studies
Electronic searches of databases
PubMed, CINAHL, Wiley Cochrane Library, and Scopus were searched to identify relevant studies using a comprehensive search strategy. The search strategy was developed using free-text and MeSH terms to retrieve eligible studies (Appendix A in the Online Supplementary Document).
Electronic searches of other sources
To ensure that all relevant studies were included, clinical trial registries, including clinicaltrials.gov and WHO International Clinical Trials Registry Platform, bibliographies of previous relevant systematic reviews, and bibliographies of all included studies were searched.
Selection of studies
All records identified by the search were imported to Covidence (Covidence systematic review software VHI, Melbourne, Australia). After removing the duplicates, two review authors independently reviewed the titles and abstracts of the studies. The disagreements encountered at this stage were resolved by consulting with a third reviewer. This process was followed by full-text screening, where the eligibility of the study was assessed independently by two review authors, and the conflicts identified were resolved similarly. We also recorded reasons for the exclusion of the studies. Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow chart was used to report the selection of the studies.
Data extraction and management
Two review authors independently completed data extraction using a standardized data extraction form in Microsoft Excel. The data extracted was compared and reviewed to identify inconsistencies or conflicts. In cases of inconsistencies, the study was reviewed again, and discussion was held to come to a consensus.
RESULTS
Results of the search
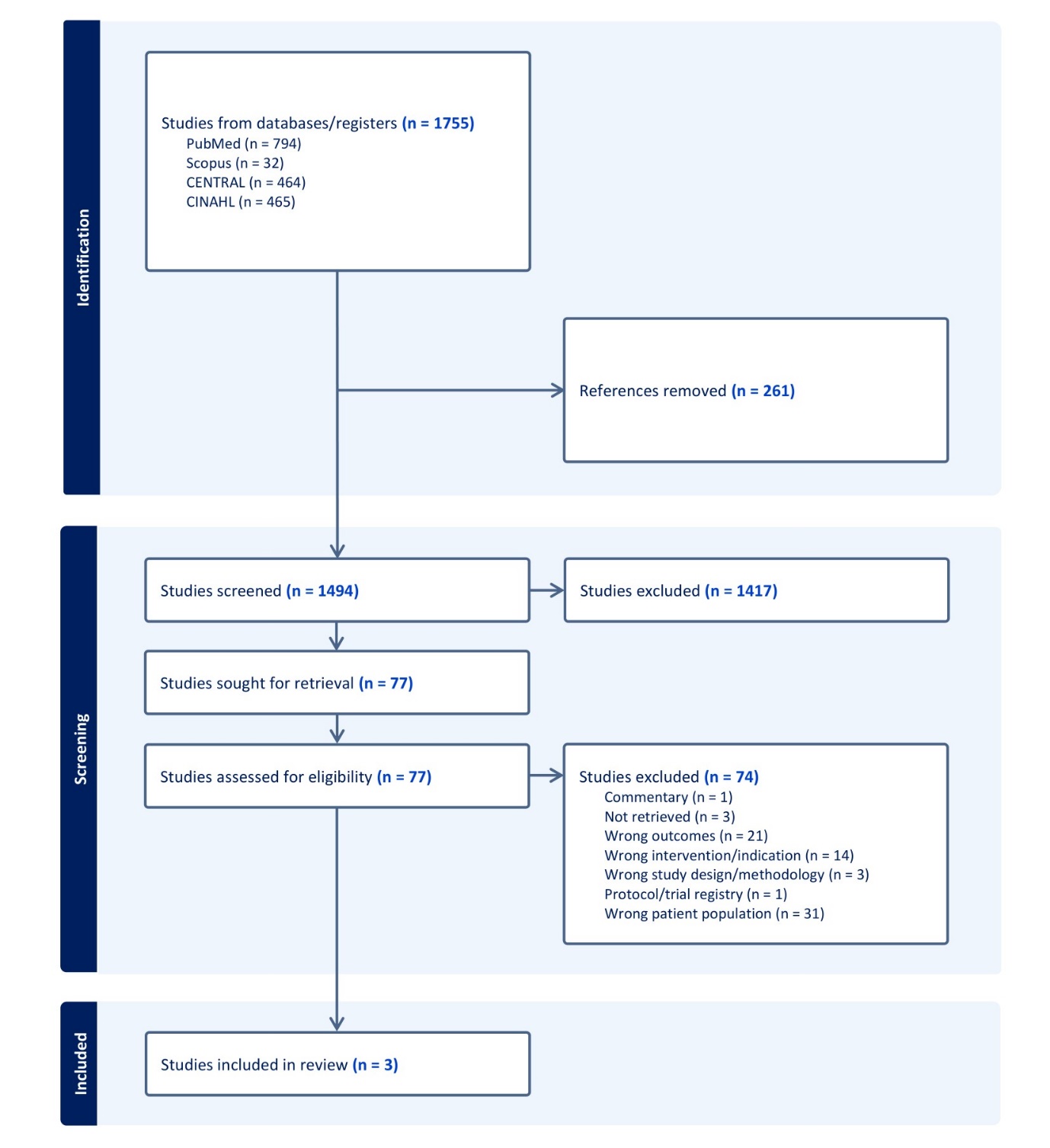
Our search across PubMed, CINAHL, Wiley Cochrane Library, and Scopus yielded 794, 465, 464, and 32 records, respectively (Figure 1). Following the removal of duplicates, 1494 studies were screened based on the eligibility criteria, excluding 1417 studies during the title and abstract screening stage. The remaining 77 studies underwent full-text screening, where all were excluded for not meeting the eligibility criteria. However, among these exclusions, three studies were identified that, while not including the intervention of interest, utilized alternate care methods compared to routine care within the population of interest – malnourished children with diarrhea. Consequently, we provide a narrative synthesis of these three studies and report a review where no studies met pre-defined inclusion criteria.
.jpeg)
Findings
Variations in the definition of alternate care across studies and the descriptive nature of our research question led to substantial heterogeneity in the findings. As a result, we were unable to conduct a meta-analysis or a quality assessment. Since no studies directly compared standard care to enhanced care in our population of interest, we did not apply a systematic grading system to evaluate the strength of the evidence.
Excluded studies
After the initial screening, 77 studies were screened for eligibility through full-text review. Out of these, around 17 studies were excluded due to wrong indications or wrong interventions, where the provided care did not involve enhanced care methods (Appendix B in the Online Supplementary Document). Additionally, around 31 studies did not include our population of interest; for example, patients who did not have diarrhea or malnourished children were excluded from the studies. Similarly, 21 studies did not include outcomes of interest; for instance, the reported outcomes were growth parameters. Furthermore, three studies with comparison groups were inappropriate for the review or had methodological limitations. In addition, three studies could not be retrieved whereas two records were of protocol and commentary.
Description of studies comparing alternate care to standard care
Study characteristics
The three studies (Appendix C in the Online Supplementary Document) were RCTs, with one study16 being a phase II RCT. Geographically, two trials took place in Asia (Bangladesh)17,18 while one in Africa (Kenya).16 All three trials were conducted in a hospital-based setting. A description of the included studies is given in Table 1.
Participants characteristics
The trials included 395 participants of either gender.16–18 One study17 included children aged 6 to 60 months, while another18 included participants from 6 to 36 months of age. Children in the third study16 were older than 6 months, with a median age of 15 months. All three studies included children with severe dehydrating diarrhea and malnutrition, with one study16 also including children with shock.
Interventions
The alternate care provided to children in these three trials included modifications to the existing WHO fluid resuscitation recommendations. Akech et al. (2010)16 compared the effect of isotonic fluids, Ringer’s Lactate (RL), with the WHO fluid resuscitation regime (half-strength Darrow’s in 5% dextrose (HSD/5D)). RL was administered as an initial bolus of 10 ml/kg over 30 minutes, with a possible twice repetition within 1 hour (up to 30 ml/kg) if clinical signs indicated any shock features. HSD/5D was given as an initial bolus of 15 ml/kg over an hour, and the bolus was repeated if improvement was noted.
The study by Alam et al. (2015)18 assessed the efficacy of modified WHO oral rehydration solution (ORS) (WHO recommended ORS with some modification, Na 75 mmol/L, Cl 87 mmol/L, K 40 mmol/L, citrate 7 mmol/L, Mg 3 mmol/L, Zn 300 μmol/L, Cu 45 μmol/L, glucose 90 mmol/L) plus partially hydrolyzed guar gum (PHGG) (15 mmol/L) compared to modified WHO ORS only. In the other trial by Alam et al. (2020),17 the children were administered intravenous fluid at different rates. The children assigned to rapid rehydration therapy were given intravenous fluid (cholera saline comprised of sodium (133 mmol/L), chloride (98 mmol/L), potassium (13 mmol/L), and bicarbonate (48 mmol/L) in the form of acetate) at a rate of 100 ml/kg over six hours. The slow rehydration therapy included infusion of 15 ml/kg of cholera saline over one hour. Rice-based ORS and a therapeutic diet were also followed.
Outcomes
Out of our main outcomes, the three trials reported treatment failure, mortality, and SAEs.
Treatment Failure
In the study by Alam et al. (2015),18 treatment failure (the continuation of diarrhea) at 72 hours was derived using the recovery outcome. Diarrhea was defined as three or more watery stools for 24 hours. In the modified ORS plus PHGG group, the proportion of participants experiencing treatment failure was lower (53.9%) than those in the modified ORS group (69.8%). However, these differences were insignificant (risk ratio=0.77, 95% confidence interval (CI)=0.58, 1.02). Alam et al. (2020)17 defined treatment failure as not achieving complete rehydration, indicated by no sign of dehydration after 6 hours in the rapid rehydration group and 12 hours in the slow rehydration group. The trial reported 3 cases of treatment failure in the rapid rehydration group compared to 2 cases in the slow rehydration group (odds ratio=1.5, 95% CI=0.2, 9.0), indicating statistically insignificant findings.
Mortality
Mortality was reported in two studies.16,17 The number of deaths reported in the RL group (9/22) was comparatively less than in the HSD/5D standard care group (13/19) (p-value: 0.11). In the study by Alam et al. (2020),17 no mortality was recorded in any of the groups.
Serious Adverse Events (SAEs)
Two out of three studies16,17 considered fluid overload as an SAE, and no cases were reported in either of the studies.
DISCUSSION
This systematic review aimed to assess the effectiveness of enhanced care in improving the outcomes for malnourished children with diarrhea with or without dehydration. Despite conducting a comprehensive literature search, we found no studies directly or indirectly addressing the review question. This lack of evidence can be attributed to the nature of the population and intervention of interest, as malnutrition and diarrhea are closely linked to poverty3 and are most prevalent in regions where even recommended care is inaccessible to a large population. In LMICs, approximately 37-54% of children have access to ORS, and only 18-20% also receive adequate zinc supplementation during an acute diarrheal episode.19 Therefore, it is reasonable to expect that most resources are allocated towards preventing or improving the coverage of essential treatment for these diseases.19
Previous studies, such as those examining diarrhea-related mortality in children with severe acute malnutrition, have noted that close monitoring is often compromised by resource limitations and a lack of skilled health professionals.11 As a result, enhanced care remains under-researched, with priority given to immediate survival interventions over complex care models. The lack of focus on enhanced care affects the current treatment protocols, which are primarily designed for short-term management. By integrating proposed components of enhanced care that are cost-effective and scalable in low-resource settings, long-term clinical outcomes of children with diarrhea and malnutrition can be significantly improved.
As no eligible studies were found using the definition of enhanced care, we broadened the research question and attempted to identify studies with alternate or supplementary treatments for diarrhea. While not meeting the specific criteria for enhanced care, the included studies provide baseline data on alternate care and allow comparison with outcomes from standard care practices in malnourished children with diarrhea. Moreover, we found three trials that compared alternate fluid regimens to the WHO recommendations in our population of interest.16–18 We also identified a few trials where an additional treatment measure was given to one group while the other group received the recommended care. These additional treatment measures included high-dose (200,000 IU) vitamin A given for 15 days,20 Saccharomyces boulardii given for an unknown duration,21 co-trimoxazole given for 6 months,22 and azithromycin given for 3 days (ABCD trial) to the intervention cohorts.23 However, these studies either did not describe the number of children with dehydration or had <80% children who had concomitant malnutrition, diarrhea, and dehydration. Some of these studies, such as the ABCD and the co-trimoxazole trials, followed patients for 180 days and up to 1 year, respectively. However, we could not extract any viable information because all patients were receiving prolonged follow-ups, and the trial did not provide baseline measures of the outcomes.
Although we anticipated a low output from this review, we did not expect to report an empty review. Similar to our study, a previous systematic review aimed to identify optimal diagnostic and treatment strategies for malnourished children with diarrhea in community settings did not report any studies. However, upon broadening their research question to include inpatient management, they identified and included 32 eligible studies.24 None of the studies in this review met our inclusion criteria of enhanced care. Additionally, a two-armed RCT that compared inpatient with day-clinic management of children with severe malnutrition and pneumonia25 and a five-armed RCT on community-based follow-up care of severely underweight children with acute infections26 reported that establishing a follow-up care system was feasible within the primary care structures.
This review has certain limitations. First, our review exclusively focused on malnutrition as a single risk factor, and the inclusion of other risk factors such as HIV, tuberculosis, and WASH indicators would have offered varied insights. Second, since this review was restricted to studies in the English language and did not include grey literature or unpublished data, we might have missed additional evidence related to the research question. Nevertheless, we believe the substantial number of studies retrieved from the databases was sufficient to address the PICO framework if relevant evidence existed. Further, we did not contact authors to retrieve studies or disaggregated data, potentially leading to the exclusion of a few studies. However, it is worth noting that the yield from contacting authors is typically low,27 and given the amount and type of knowledge we required, we believe that our output would likely have remained low from such efforts.
CONCLUSIONS
Our review highlights the lack of direct or indirect evidence comparing standard care practices with enhanced care. We learned that enhanced care in managing diarrhea and malnutrition is relatively understudied, emphasizing the need to generate evidence in this area. Moreover, future reviews that focus on additional risk factors, such as HIV and age, are imperative to establish conclusive evidence regarding the effectiveness of enhanced care in managing children with diarrhea.
Funding
This work was funded by a grant (203171754-1) from the World Health Organization (WHO) grant to the Centre of Excellence in Women and Child Health, Aga Khan University (AKU). Employees of WHO contributed to the design, review, and technical input.
Authorship contributions
SS, SA, YBN, and JKD conceived the study and initiated the study design. UJ, AK, and AS led the conduct of searches. RA, KV, AK, UJ, AI, and AM conducted the data extraction. RA, UJ and AK performed data analysis. RA, KV, AK, UJ, AI, and AM critically reviewed the manuscript. All authors contributed equally to the revisions and approved the final manuscript.
Disclosure of interest
The authors completed the ICMJE Disclosure of Interest Form (available upon request from the corresponding author) and disclose no relevant interests. YBN is a staff member of the World Health Organization. The authors alone are responsible for the views expressed in this article, and they do not necessarily represent the views, decisions, or policies of the institutions with which they are affiliated.
Additional material
The article contains additional information as an Online Supplementary Document.
Correspondence to:
Shabina Ariff
Professor
Department of Paediatrics & Child Health
Aga Khan University
National Stadium Road, Karachi, Sindh
Pakistan
shabina.ariff@aku.edu