INTRODUCTION
The World Health Organization (WHO) advises breastfeeding exclusively for the first six months of a child’s life to promote healthy growth and development. The benefits of exclusive breastfeeding (EBF) for child development should have been added to the editorial.1 According to WHO 2023, breastfeeding is one of the most effective ways to maintain health and ensure child survival. Breast milk is the ideal food for infants. It’s safe, clean, and contains antibodies that protect against many common childhood illnesses.
Breast milk provides all the energy and nutrients an infant needs during the first six months of life and continues to cover half or more of its nutritional needs during the second half of life and up to a third of those. this during the second year. Children who have been breastfed perform better on intelligence tests and are less likely to suffer from overweight, obesity or diabetes later on. Additionally, women who breastfeed have a lower risk of developing breast or ovarian cancer.1
This low membership rate in the EBF is attributed to several factors, which vary somewhat depending on the nation.1–3 Breastfeeding compliance is still a big issue in several of the Democratic Republic of Congo, DRC’s health zones. The Democratic Republic of Congo’s 2013–2014 Demographic and Health Survey, which is nationally representative, indicates that less than 50% of infants are breastfed exclusively.
Breastfeeding is common in the capital city of Kinshasa, but one in five newborns received something else during their first three days of life, 53.5% of children ages 6 to 23 months have an EBF, per the multiple indicator cluster survey (MICS)-DRC 2017–2018 survey report.2 These national percentages are much higher than the province-by-province and even within-province percentages in the different health zones.
A 2014 study conducted in Kinshasa by Babakazo et al. found that 2.8% of children were exclusively breastfed until they were six months old.3 Sustainable Development Goal, SDG, 2 stipulates that the EBF component must have a rate of at least 50%. According to the Monitoring Improved for Action (MAA) survey conducted in 2013-2014,4 only 13.7% of children aged 0-6 months were exclusively breastfed, well below the 50% target set by SDG 2.
The Hospital data from the Health Zone encoded in the data encoding software in the health zone demographic health information system (DHIS2) over the last two years show low rates of exclusive breastfeeding: 23% in 2021 and 28% in 2022. The WHO and United Nations Children Fund (UNICEF) are encouraging breastfeeding by distributing the “10 conditions for successful breastfeeding”4 as part of the “Baby Friendly Hospitals” Initiative (BFHI). Furthermore, breastfeeding is crucial in the global strategy for feeding newborns and early children.4 Despite several international initiatives, exclusive breastfeeding rates (EBF) have remained unchanged for the past twenty years. The Dibaya health zone in the DRC is one of the environments where adherence to EBF has not improved despite a number of studies being conducted to identify various obstacles and barriers to the practice
The current study aims to explore the various factors contributing to the low rate of EBF adherence in the DRC, specifically in the Dibaya health zone. The goal is to raise this rate of EBF adherence, lower the morbidity and mortality rate of children under five in the Dibaya Health Zone, and enhance the health of infants and young children.
METHODS
Study location
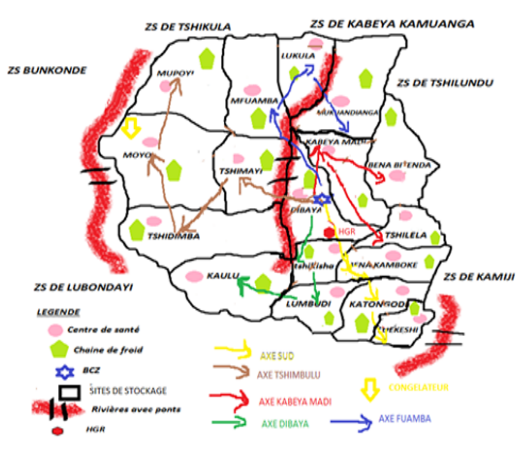
The study took place in the Dibaya health zone in the Kasai Central province. It is a post-conflict zone of Kamuina Nsapu from 2017-2018. We note low agro-pastoral production, leading to a large number of children suffering from malnutrition (with 45% of stunting according to MICS 2018), low schooling for girls in favour of boys; food prohibitions among pregnant women, a negative influence on the EBF by grandparents, parents, mothers-in-law and husbands who introduce other foods early into the children’s diet.
.png)
Sampling
This is a cross-sectional study carried out among women breastfeeding children aged 6-23 months living in Dibaya during the study period. Two statistical units were sampled using a two-cluster probability method, namely lactating women/caregivers of children aged 6 to 23 months and children aged 6 to 23 months living in households.
The proportion formula was used to determine the sample size. We used the 13.8% prevalence from the 2013–2014 MAA survey. N ≥ ((1.96) ^2*0.138*(1-0.138))/ 〖 0.05^2 =182.7, or 183 mothers and caregivers of children between the ages of 6 and 23 months, was the sample size.
Following a 10% increase to account for refusals and non-responses, the sample size was lowered to 201 mothers and caregivers of infants aged 6 to 23 months.
We used a four-stage probability sampling procedure, the Dibaya health zone was first carefully chosen based on the study’s location.
The health zone at the second level has 17 health areas (AS), including 2 urban and 15 rural AS. Two urban AS will be chosen automatically from the list of AS, and seven rural AS will be chosen randomly from the list of fifteen rural AS.
At the third level, streets and villages make up each AS. Three streets/villages were selected randomly from the list of streets that included each AS to be examined after all the streets/villages had been listed.
At the fourth level, a pilot survey was conducted in each chosen street to compile a list of plots with at least one household with a child between the ages of 6 and 23 months.
Then, based on the weighted size of each health area, a random drawing was conducted to select which households were to be surveyed.
Only one child, ages 6 to 23 months, was chosen from each household of children (if there are more than one, then one can be chosen by a simple random draw).
The mother of the child, between the ages of 6 and 23 months, or the child’s caregiver will be interviewed in the selected household.
Data collection
We used the structured interview technique using a survey questionnaire administered to breastfeeding women with children aged 6-23 months. After obtaining authorization from the ethics committee of the Kinshasa School of Public Health (KSPH) and that of the political-administrative and health authorities at the local level, the investigators were searched and briefed on the collection methodology with Kobo collect. Then, a pretest was carried out in a non-selected health area. After correcting the questionnaire, we began the collection itself.
Analysis
The data were gathered, sent to the server, and then imported into SPSS version 26.0 with the assistance of structured interviews based on a Kobo collect survey questionnaire given to nursing women with children aged 6-23 months.
Quantitative data were presented as mean with standard deviation or median with interquartile space, depending on whether the distribution was normal or abnormal.
Qualitative data were summarised in absolute and relative frequency. The chi-square test showed the current relationships between EBF adherence and various factors, and the relationship between the various factors will ultimately be ascertained through logistic regression.
Ethics
The study protocol received approval from the KSPH ethics committee and authorization from the political-administrative authorities of the Dibaya Territory. After a brief explanation of the study’s purpose, each participant was asked to give informed consent to participate. The data collected is classified confidential; only the research team is authorized to access it.
No preference was given to the participants in this study in relation to belonging to a specific socio-economic level or others.
RESULTS
Sociodemographic and sociocultural characteristics of the mother of children aged 6-23 months
Table 1 indicates that the mother’s median age was 27 years, with an EIQ of 11 years. Almost 25% of mothers with children between the ages of 6 and 23 months were under 27, and the majority of respondents were married. Additionally, 7 out of 10 respondents were from rural areas, more than half of them were farmers, more than a quarter were Catholic, and nearly three quarters had a monthly income of less than 200,000 Fc.
Table 2 indicates that in 11.1% of cases, there were cultural or familial reasons, and in 4.5%, there were tribal rules.
Sociodemographic and clinical characteristics of children aged 6-23 months
According to Table 3, eight out of ten children had birth weights greater than 2,500 grams, the median age of weaning was six months, with nearly nine out of ten children who were weaned before six months, and nine out of ten children who were surveyed were still being breastfed. More than half of the children were girls.
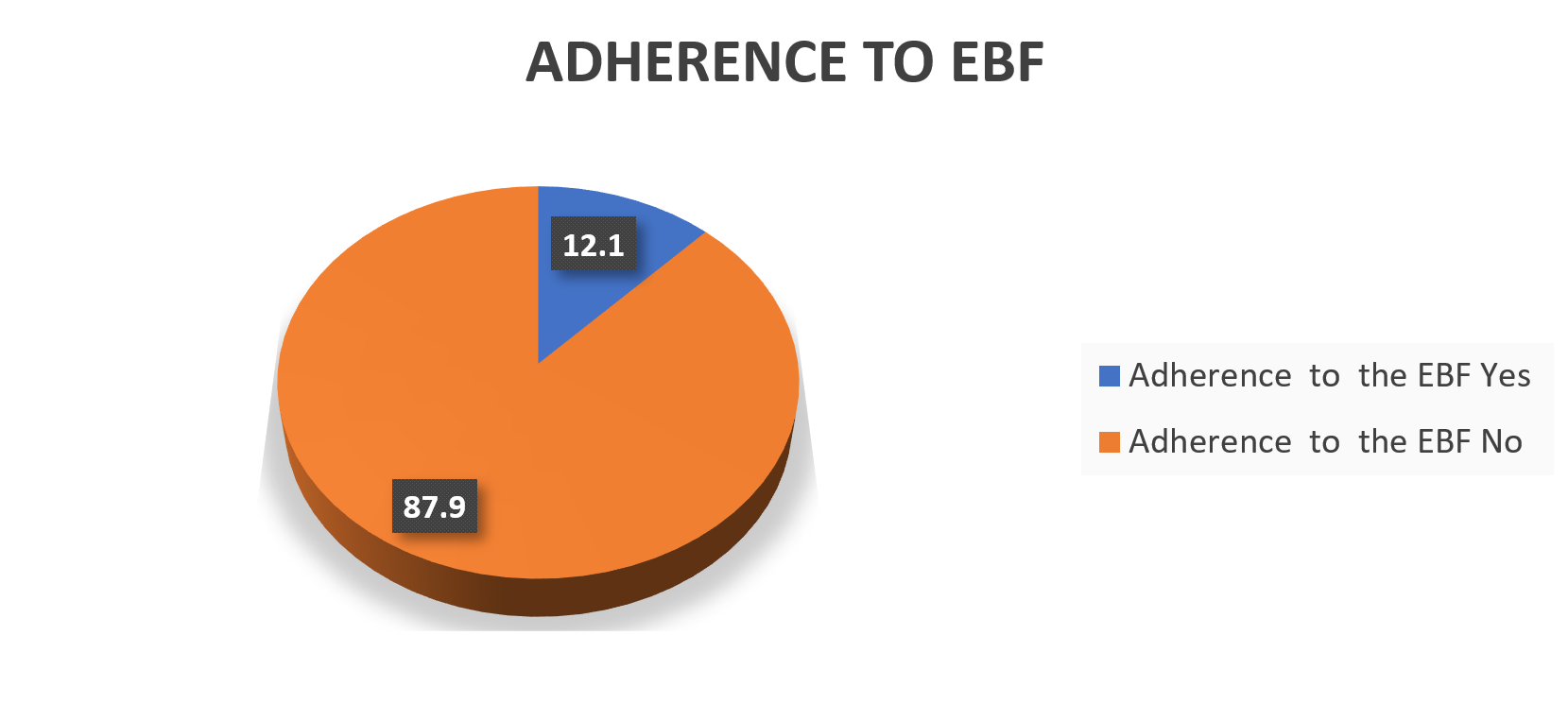
Adherence rate to the EBF in the Dibaya ZS

Figure 2 shows that 9 out of 10 mothers of children between the ages of 6 and 23 months did not enroll their child in the EBF during the first 6 months of life.
Table 4 shows that 9 out of 10 mothers of children between the ages of 6 and 23 months did not enroll their child in the EBF during the first 6 months of life, 7 out of 10 breastfed their children on demand, and 25% did not because they did not have enough time to breastfeed. The majority of these mothers cited being too busy with their jobs or fieldwork as reasons for their lack of time.
Knowledge, attitudes and practices of mothers on EBF
According to Table 5, nine out of ten mothers were aware of EBF; 81.4% had learned about it from healthcare professionals during CPN/CPS, and 63.7% had learned about it from Reco; over half of mothers had breastfed their newborns immediately; 11% had given them a solution before their milk came in; and 12.1% of mothers had exclusively breastfed their children for the first six months of their lives.
Factors associated with non-adherence to the EBF
After applying the Chi-square test, Table 6 shows that the woman’s occupation, marital status, place of residence, and the health area’s location are all statistically related to her adherence to the EBF.
Table 7 (after applying the Chi-square test) shows that the existence of rules/prohibitions in the tribe is the only socio-cultural characteristic associated with adherence to the EBF.
Table 8 suggests that adherence to the EBF statistically correlates with the knowledge already acquired.
DISCUSSION
Rate of adherence to exclusive breastfeeding (EBF) among mothers of children aged 6 to 23 months in the Dibaya Health zone
The study’s findings show that a quarter of the participants did not have enough time to breastfeed their children; of those who did, the majority cited being overly busy at work or in their field activities; nine out of ten were still breastfed; nearly nine out of ten were weaned before the age of six months; nine out of ten had taken a food other than breast milk before the age of six months; and seven out of ten breastfed their children on demand.
The WHO goal of having this rate surpass 50% of the EBF rate by 2025 is still far off. When comparing these findings to those of other studies, we observe that the rate is significantly lower than that of the MICS-RDC-2018 survey, which found 53.5% at the national level and 47.6% at the provincial level, as well as the Pronanut 2023 national nutrition survey, which reports a national EBF rate of 59.6% and 45% at the provincial level (Kasai central).5
According to Elias Bashimbe Raphaël et al. study,2 69.3% of South Kivu residents exclusively breastfed their children for up to six months. This could be explained by the fact that the study was conducted in a military camp in the South Kivu province, particularly considering the recent improvements in camp care, which also show that the rate of exclusive breastfeeding (EBF) meets the WHO’s threshold for achieving the SDGs, which state that by 2025, the rate of EBF should be above the 50% threshold.
Given that over 75% of mothers in the Dibaya health zone do not exclusively breastfeed, it is critical that all segments of the community participate in the creation of an awareness-raising program, especially for women who are childbearing. propagate the advantages of breastfeeding exclusively for the first six months of a child’s life, thereby lowering the percentage of EBF non-adherence.
Knowledge of mothers of children aged 6 to 23 months in the Dibaya health zone on the EBF
The study’s findings show that nine out of ten mothers were aware of EBF; 81.4% had learned about it from medical professionals during CPN/CPS and 63.7% from Reco; more than half of mothers had breastfed their infants exclusively for the first six months of life; 11% had given their kids a solution before their milk came in; and 12.1% of mothers had given birth to their children.
Out of the 260 women questioned in the study by F. Ben Slama,6 41.5% exclusively breastfed, and 58.5% used artificial milk either alone or in conjunction with breast milk. When it came to the guidelines for breastfeeding, the best time to stop breastfeeding, and the key foods to start introducing when diversifying infant feeding, first-time mothers’ knowledge, attitudes, and behaviors were inadequate. This may be caused, among other things, by moms’ lack of knowledge and education, as well as occasionally by the absence of the essential tactics for EBF promotion in this health zone.
Factors associated with non-adherence to exclusive breastfeeding
The type of health area the mother lived in (p=0.001), her marital status (p=0.006), her area of residence (p=0.001), her occupation (p=0.03), the presence of rules or prohibitions in the tribe that affect the EBF (p=0.049), and the mother’s knowledge of exclusive breastfeeding (p=0.045) were among the factors linked to non-adherence to the EBF.
In the systematic review by Kavle, sixteen obstacles to EBF were found, including data showing a negative correlation between maternal employment and EBF practice. Additionally, there was strong evidence found regarding the mode of delivery, indicating that caesarean sections can negatively impact the EBF, particularly during the first week. Improvements in adherence to EBF were shown when family and/or community support was present, along with EBF counselling. These findings contrast with NR Diagne-Guèye et al.,7 who discovered that socio-cultural representations caused mothers to feel the need to add additional foods, which some mothers (36%) found to be crucial to administer.
This implies that habits and customs should be considered as contributing factors to following the EBF. In the context of our research, habits and customs are crucial in combating various health issues, particularly in rural areas. Reducing infant and child mortality would be achieved by addressing this factor through awareness-raising, social and behavioural change communication, and education about the advantages of exclusive breastfeeding during the first six months of life.
Implications
In view of the results, it is necessary to train providers in the Dibaya Health Zone in the Baby-Friendly Hospital Initiative to influence breastfeeding women’s knowledge of the importance of EBF. Intensify awareness of EBF by involving community leaders, customary authorities as well as the husbands of breastfeeding women. Create income-generating activities to empower women, especially in rural areas in the Dibaya health zone. Communication for behaviour change must also focus on the age at which complementary foods are introduced. Health sector partners should finance initiatives to improve and promote EBF in this health zone to reduce child mortality due to malnutrition. The use of expressed breast milk and its storage should be considered in other future research as a viable option to help mothers maintain the breastfeeding chain and overcome barriers posed by labour.
CONCLUSIONS
In the current state of affairs, breastfeeding is still a very complex act that is the most natural and beneficial that is hard to replace. The Dibaya HZ continues to have low EBF adherence (12.1%), and the majority of mothers do not follow exclusive breastfeeding guidelines. This is concerning and needs to be addressed as a key issue. Other than breastfeeding, no other intervention has such a substantial impact on the infant’s current and long-term health. It is for this reason that exclusive breastfeeding must be strictly obligatory for any woman with a child under 6 months old.
The work of breastfeeding mothers constitutes a significant barrier to adherence to exclusive breastfeeding (EBF). Therefore, policymakers should adopt laws that will promote the practice of EBF by working mothers, such as extending maternity leave and creating laws that allow working mothers to breastfeed while they are at work.
In particular, educate mothers about the advantages of exclusive breastfeeding for the first six months of a child’s life. Changing social norms and behaviours through communication about the benefits of exclusive breastfeeding can also be a useful strategy to reduce infant and child mortality caused by noncompliance with the EBF.
Acknowledgements
To the steering committee of the Kinshasa School of Public Health and to Professor Godefroid Musema for their support throughout the process.
Funding
None
Authorship contributions
Emile Mbuyi designed the entire study, conducted the data collection, and wrote the master’s thesis, which is the basis for this manuscript. Bernard-Kennedy Nkongolo contributed to the analyses and discussion. Musema Godefroid supervised and facilitated the entire process of producing this dissertation as part of completing the Master in Public Health. She evaluated the different versions of the dissertation protocol and gave guidance on the manuscripts.
Competing interests
The authors declare no competing interests.