Introduction
Spending on healthcare is one of the parameters that determines the economic growth of a country or region. It is an investment in human capital that affects economic growth.1 There is a correlation between a country’s economic power and the level of healthcare spending: the richer the country, the higher the proportion of Gross Domestic Product (GDP) devoted to healthcare.2 As a result, the total GDP and GDP per capita have a significant influence on life expectancy.3 The latter is one of the indicators of healthcare systems and economic development.4
Surgery is an essential link in the healthcare system, which is defined as “all organizations, people, and actions whose primary interest is to promote, restore, or maintain health”.5 Inadequate access to surgical services results in unacceptable morbidity and mortality from a variety of health problems, particularly for marginalized segments of the population in low- and middle-income countries.6 The burden of surgical disease is enormous and growing,6 so it is necessary to strengthen surgical care within health systems.7 This requires training and equipment. With the progress of science, the use of medical technology and information technology has become almost constant in surgery, and in urology in particular. This affects costs, quality of care and, consequently, patient safety.8 Modern urological practice is based on endoscopy (endourology), laparoscopy, and robotic surgery, which is beginning to occupy a place in developed countries. Endourology encompasses a variety of minimally invasive techniques, most often performed through natural orifices, with excellent surgical and postoperative results. Its practice requires a certain level of equipment and technical skills. In Africa, it is often reported that the lack of equipment and technology in the healthcare system still imposes the practice of open surgery in a large part of the continent. In a pan-African survey conducted by the association Modern Urology For Africa,9 it was reported that “In some African countries, endoscopic urological surgery is either in its infancy or not yet performed”, and that cooperation could play an important role.
Regarding the various aspects described above, the authors of this article propose to carry out a review based on data collected from African centers. Based on the literature, the objective is to define the impact of the Gross Domestic Product (GDP) on the practice of endourology and minimally invasive surgery in urology, and the role of international cooperation.
1. From global health to global surgery
One of the key objectives of the 2030 Agenda of the United Nations is the need to strengthen health systems to reduce global mortality and morbidity and achieve health equity. Health has been objectively targeted in the Sustainable Development Goals (SDGs). To achieve this health-related objective, the chosen strategy is based on a horizontal, cross-sectoral systems approach.10 This leads to transnational actions and goes beyond any geographical limits11; thus involving power and politics.12 So, beyond health at the level of the individual, it is a question of action and policy that must be carried out at the level of the population: the defining concept of global health.13 Over the past few decades, this concept has led to the creation of numerous international programs, most often aimed at eradicating or reducing a disease. As a result, surgical care has received low priority in some of the poorest regions in the world.14 This is why, in 2008, Paul Farmer considered surgery to be the “neglected stepchild of global health” in low- and middle-income countries.15 In 2015, an appeal alerted the world’s global health and political decision makers. Meara et al.16 published the following figures in Lancet Global Health: In times of need, 5 billion people do not have access to safe and affordable surgical and anesthesia care; 143 million additional surgeries are needed every year in low-income countries to save lives and prevent disability. Due to the cost of surgery and anesthesia care, 3 million people face catastrophic healthcare expenses every year. They added: investing in surgical services in low-income countries is affordable, saves lives, and promotes economic growth. The beginning of a new era, that of global surgery. It has been defined as the study and practice of improving access to timely, quality and affordable surgical care for all.17 That is why Kim et al.,7 considered surgery to be “an indivisible, indispensable part of health care”.
2. Public health spending and disparities in care in Africa
Compared to other regions of the world, public spending on healthcare in Africa remains low.18 This disparity is a major concern for African policymakers. They face a dual challenge: improving health status and reducing inequalities in health outcomes.19 The countries of the Maghreb have seen a significant improvement in the health status of their populations, while progress in sub-Saharan Africa has been slow.18 When it comes to surgical care, the level of provision is directly related to several determinants. These include public health, public finances, education, innovation, and technology.20 Added to this are internal conflicts and poverty, which are the source of real variations in health outcomes between countries and regions.18 Africa’s healthcare systems are weak and underfunded. In 2013, health financing in Africa represented only 1% of the rest of the world.21 Thus, financial inclusion must be deepened to improve the health of the population in Africa.22 In 2001, at a conference of African Union Heads of State in Abuja, it was decided to allocate at least 15% of their annual expenditure to health (known as the Abuja Conference).23 In a 2018 assessment, only two countries met this health budget target.24
3. Data and Interpretation
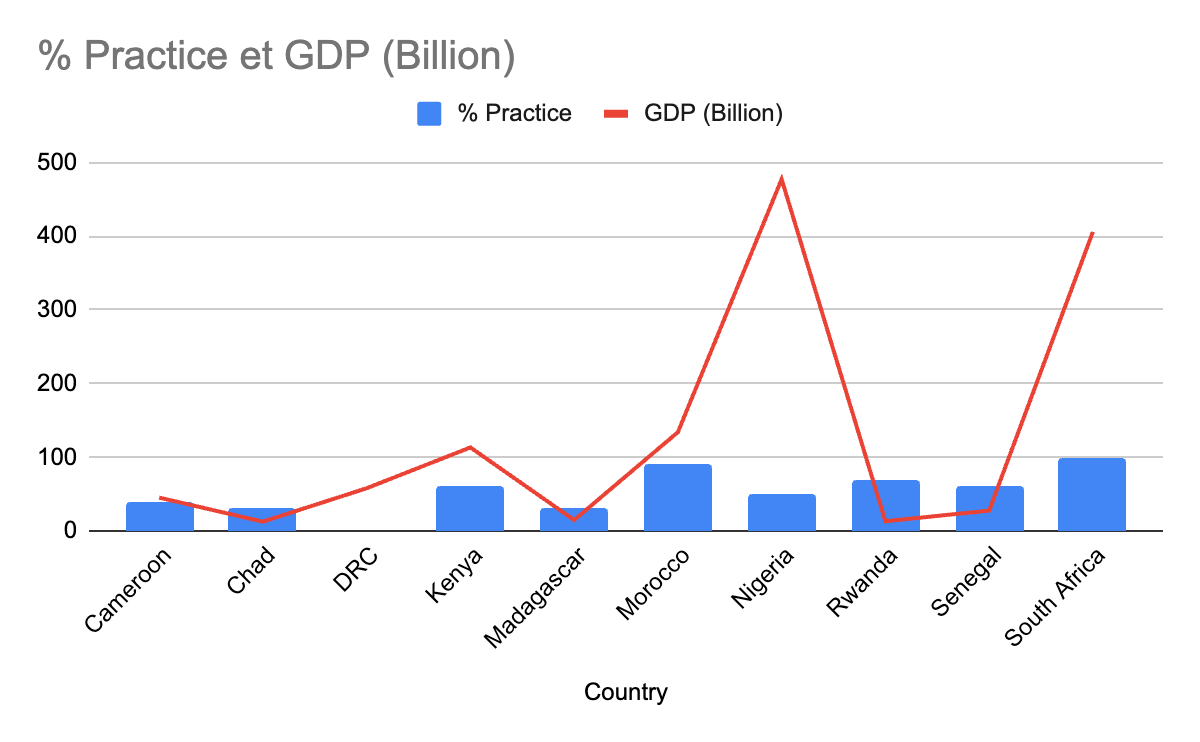
Based on data from a survey conducted in several African countries, the authors assessed the practice of endourology in 10 countries from 5 geographical areas of Africa (Table 1). This evaluation focused on the equipment and practice of endourology and laparoscopic surgery in urology. Endourology and urological surgery each accounted for 50% of the score. For endourology, 5 procedures were identified overall (cystoscopy (CS), endoscopic internal urethrotomy (EIU), transurethral resection of the prostate or bladder (TUR), ureteroscopy (URS), and percutaneous nephrolithotomy (PCNL). Each procedure had two scores: 0% if not performed in the center and 10% if performed. For laparoscopy, the 5 procedures considered were: pyeloplasty (PP), laparoscopic radical nephrectomy (LRN), promontofixation (PF), cystectomy (CP), and prostatectomy (RP). Each laparoscopic procedure was scored at 10%. GDP data were consulted on the World Bank’s official website (https://data.worldbank.org/indicator/NY.GDP.MKTP.CD on November 24, 2023 ).
.png)
Review based on real data.the x-axis is represented by GDPs, thus evolving in an increasing manner from the GDP of Chad (12.7 billion) to that of Nigeria (477.39 billion). The y-axis is represented by the percentage of gestures made. Overall, the curve evolves in a sawtooth pattern, with two main sections: the first between Chad and the Democratic Republic of the Congo and then from the Democratic Republic of the Congo to Nigeria.
In the first part, there is no correlation between GDP and the level of endourology and laparoscopy practice. DR Congo has the highest GDP but the lowest level of practice. This may be explained by the fact that the center evaluated in DR Congo (Cliniques Universitaires de Lubumbashi) is not located in the country’s main city. In Africa, most of the effort invested in health care is concentrated in the centers of the major capitals, and there is mainly one national reference center in the capital. We note that in Rwanda, the practice is at 70%, while the GDP is significantly lower than in Senegal, Cameroon, and DR Congo. This could be due to a general policy of development. The Kigali University Hospital is the oldest and largest: the national reference center. What is more, the center is located in Kigali - one of Africa’s top-rated cities.
In the second part (after DR Congo), all countries have a GDP in excess of 100 billion. The average use of minimally invasive techniques is more than 70%. In the first part, the average was below 40%. In Nigeria, the level of this practice was 50%, lower than in other countries with a lower GDP (Kenya and Senegal). The reason for this is similar to that given for DR Congo in Part I. The level is significantly higher in Morocco and South Africa. If Nigeria’s first hospital (Lagos University Teaching Hospital) had participated in this survey, perhaps the level of reported practice would have been well above 50%.
After this argument, the observation seems obvious. We observe a high presence of endourological and laparoscopic practices in countries with a high GDP and also in countries with a strong development policy.
After this argument, the observation seems obvious. We observe a high presence of endourological and laparoscopic practices in countries with a high GDP and also in countries with a strong development policy.
4. Overview of global urology in Africa and elsewhere some: literature-based overview
Surgical conditions account for between 11% and 30% of the global burden of disease. This figure is constantly increasing. In the case of urological diseases, the greatest regional increase will be in Africa. This is related to the increase in life expectancy and the rapid growth of the African population. Therefore, it is essential to improve access to sufficient urological interventions.25 In 2015, there was 1 urologist per 2.3 million inhabitants of Zambia.25 In Nigeria, this ratio is 1 urologist per 3.2 million inhabitants.26 In a study of the burden of urological disease in Malawi, Juvet et al.27 concluded by emphasizing urological training in sub-Saharan Africa. This argument is advanced by many authors.9,26 In addition to this, emphasis is also placed on equipment funding.26,27 The practice of open surgery still occupies an important place. In a survey of several public centers in Africa, open surgery is the surgical management procedure used for the management of kidney stones in 57.1% of cases and in 52.3% of cases for the treatment of complicated benign prostatic hypertrophy.9 In Nigeria, for example, few public hospitals offer basic endourology, with most procedures performed in private facilities.28 Although in low-income countries the adoption of endourology is low and open surgeries are still widely practiced, minimally invasive and endourological procedures for the treatment of urological diseases are commonly practiced in high-income countries.29,30 It should be noted that the practice of endourology and minimally invasive surgery brings safety to both the patient and the surgeon. It has a significantly lower morbidity and mortality than open surgery and offers rapid recovery and early return to activity.
5. The Challenges of Minimally Invasive Surgery in Africa and the role of international cooperation
For health systems to be strengthened, especially for sustainable development, it is essential to place particular emphasis on service delivery capacity.31 That is why, in order to fill and assess the gaps in healthcare systems in terms of surgical care worldwide, the Lancet Commission proposed six indicators.17 These indicators have been adopted by the World Bank Group as part of its development indicators.32 One of the main indicators is the density of specialized surgical personnel. In Africa, the density of surgeons in general and urologists in particular is low.26 In addition to the low density of urological specialists, there are other factors that influence the practice of endourology and minimally invasive surgery, which remains low. Today, open surgery is still performed in referral centers.9 International cooperation can play a major role in changing current practice. This is why several UN agencies (World Health Organization, United Nations Institute for Training and Research, United States Agency for International Development, etc.) and regional agencies (South African Development Community, South Asian Association for Regional Cooperation, Caribbean Community, etc.) are working to develop global surgery.14 There are societies or associations that operate exclusively in the field of urology. IVUmed, Urolink,33 the Société Internationale d’Urologie,34 etc. This type of cooperation can focus on training and equipment reinforcement. Off-site training, in highly developed centers, can have certain disadvantages: very different disease management and an unsuitable care environment.35 Afrocentric models are needed and the surgical oncologist should be at the heart of this system.36 This cooperation in developing sustainable urological services must be based on understanding local needs and appropriate training that is easy to impart in local centers. which can be perpetuated and spread throughout a region in need.35 Reference training centers can be set up and run regionally. In this way, they can be oriented and adapted to the local context. They can also be easily relocated and better evaluated. Equipment support can be provided in accordance with local needs and, above all, maintenance capacity.
Conclusions
The practice of endourology and minimally invasive surgery imposes a certain requirement, namely the availability of qualified personnel and suitable equipment and consumables. This practice seems to be linked to the level of economic development of a country. It is well established in centers in countries with a high GDP. However, practice is possible in low- and middle-income countries with the commitment of political will and international cooperation.
Funding
This project has not received any funding
Authorship contributions
The authors all played a substantial part in this project, from draft, design and final version.
Disclosure of interest
The authors declare that they have no conflict of interest.
Correspondence to
Saleh Nedjim, Modern Urology For Africa[1], Casablanca, Morocco. Email : nedjimsaleh@gmail.com, nedjilsaleh@mufafrica.com
A non-profit association registered in Morocco, dedicated to developing the practice of endourology and minimally invasive urological surgery in Africa.