Globally, most deaths occur during the postpartum period due to several factors, one of which is the availability of facility-based to address complications1–3 Pondering the necessity for improving the quality of care for maternal and neonatal health becoming a global priority.4 The World Health Organization’s (WHO) vision for the quality of maternal and newborn health focuses on three essential domains required for the quality of care such as dignity and respect, communication, and emotional and mental support.5,6 Though the world has achieved significant improvements in reducing maternal mortality, the situation is still not optimal in terms of the quality of healthcare delivery in government health facilities, leading to maternal health, which remains a significant public health problem worldwide.
Substantial recent studies conducted in India reported women’s experiences of mistreatment and disrespect while delivering a baby in health facilities.7–9 A literature review conducted to synthesize the prevalence and factors leading to abusive treatment during childbirth in India shows that around 20% of women experienced any form of disrespect from healthcare providers during childbirth in health facilities.10,11 However, behavior such as physical abuse and non-consented care was highly reported in most of the studies. The majority of studies reported varied forms of mistreatment such as physical abuse, abasement, verbal abuse, non-consented medical processes, lack of privacy, lacking knowledge or information, denial to give pain relievers, gross assault of confidentiality, denial of admission to health facilities, being ignorant to women during childbirth to suffer life-threatening, avoidable aftereffects, and restraining of women and their new-born in facilities after childbirth due to an inability to pay.12–15
A considerable number of studies have focused on defining mistreatment and disrespect in various geographical settings.12,13 Few studies also focused on contextual factors, system-related factors, and providers’ behavior while providing quality care during childbirth.1,7,14 Lack of health care infrastructure, human resources, and overcrowding leads to the burden on existing human resources in the facilities leading to disrespect and mistreatment. Health facility-related factors are mediating factors that escalate the behavior of healthcare providers.
Globally, literature shows that women experienced mistreatment and disrespect during delivery in health facilities in low and middle income countries (LMICs). A cross-sectional study conducted in a hospital in eastern Ethiopia showed an association between the respectful maternity care received by the women at the time of labor and delivery. The study concluded that providing women-friendly, abusive-free, timely, and discriminative-free care can improve and increase the uptake of institutional deliveries. The study suggested that women-centered services could substantially reduce maternal mortality.16 Similarly, another study focused on overcoming the barriers to safe motherhood. The study discussed disrespectful and abusive maternity as the prevalent problem that disproportionately impacts marginalized women. The study proved obstetric care navigation; a new approach can help mitigate the disrespectful and abusive treatment a delivery woman receives during labor.17
Another direct observatory hospital-based study conducted in the public care facilities of Gujarat again talked about the disrespectful care being a barrier to pregnant women and their families accessing healthcare services. A cross-sectional study was conducted across public facilities (PHC, CHC, and district hospitals); the direct observation tool was developed to assess respectful maternity care based on different parameters. The study proved that no RMC practices are followed at any of the public care facilities. The study suggested that training primary, secondary, and tertiary healthcare workers can change the scenario with positive intrapartum care experiences and potentially increase maternal care facility uptake. The study also discussed that more research needs to be done to understand the local context of RMC, social norms, and patient-provider relations.
Current study
India has progressed in reducing maternal mortality in the last decade, indicating the impact of several health programs launched by the government. A sharp increase has been seen in antenatal care services, institutional deliveries, and post-natal care utilization. These increasing trends of maternal healthcare utilization have promised to save women and children from several life-threatening complications during childbirth. However, along with increased utilization of healthcare services, there have been several challenges in the public healthcare system while delivering quality care, respectful maternal care, and dignified care. Several factors, such as lack of human resources, lack of instruments, operation theatres, lack of beds at some times, and high patient load on health providers, hinder the delivery of quality and respectful care during facility-based delivery. Along with facility-based factors, healthcare providers’ attitudes and health seeker backgrounds also contribute to the poor quality of care during childbirth.
Pregnant women living in slum communities in urban areas experience multiple deprivations such as women from poor socio-economic statuses, living in slums, lack of availability of documents, migrants, and women. Due to this, women from urban slums go to public health facilities for deliveries and often face discrimination and mistreatment during childbirth. Recently researchers have paid attention to the issue of physical abuse, mistreatment, and disrespect during childbirth. However, Most studies have been undertaken in hospital settings, with a few using community-based approaches. However, there is a lack of research investigating women’s experiences living in slum communities in urban areas of India. Hence, the current study seeks to report abuse and disrespect during childbirth in public health facilities in urban areas.
METHODS
Study Design
A community-based cross-sectional study was conducted in the urban slums of Pune city, one of the largest agglomerate metropolitan cities in the Maharashtra state of India. Pune Metropolitan Region consists of Pune city and suburbs of Pimpri-Chinchwad of which Pune city comprises the Pune Municipal Corporation (PMC), well known as Pune Mahanagar Palika. It is the civic body that governs Pune. PMC consists of 154 administrative wards further divided for decentralized planning and functioning in the city. An estimated population of 3.99 million, and at least 40 % of the population resides in slums.
Sample Size and Sampling
Based upon the limited evidence of the mistreatment during childbirth and with the absence of data available on the estimation of how common the mistreatment of women is prevalent during childbirth worldwide, the research study was conducted. Applying simple random sampling a sample size of (n=260) recently delivered women were recruited from low-income communities in Pune city India. The urban slums were chosen based on the fact that this population is often neglected population and usually prefers public healthcare facilities to private ones due to a lack of financial resources. Therefore, the study sample size included only those women from the slum community who had delivered 18 months before the survey to avoid recall bias. The household survey was conducted by trained researchers interviewing an individual from each house. Before initiating the survey, a pre-test was conducted to check the authenticity and appropriateness of the questionnaire developed.
Inclusion and exclusion Criteria
The study included only those women respondents who delivered 18 months before the survey and those who had strictly delivered in any of the health facilities. Home deliveries were strictly excluded from the study as it failed to fit into the required criteria.
Independent Variables
Independent variables included maternal age at pregnancy (<24,>24 ), occupational status of both respondents, wealth quartile; educational level of both respondent caste (Open, Other Backward Class; OBC, Scheduled Caste; SC, Scheduled Tribe; ST, and other), religion (Hindu, Muslim, Other), gravida, gender of the child(male, female).
Dependent variables
Varied types of mistreatments and abuse such as physical, ver bal, non-consented, non-dignified, non-confidential, and abandonment of care factors, were drawn. Discrimination based on different factors such as race, ethnicity, or lack of capability to pay; physical abuse; verbal abuse; threat; lack of provision of information; ignorance or abandonment of patients who are in need; being left all alone; denial of the comfort of the patient while delivering; restrictions to the birth companions; and bribes for better care.
Qualitative data collection analysis
For the qualitative study, 15 respondents were chosen among those who had the greatest experiences of disrespect and abuse during childbirth and were willing to share their experiences by being part of the study. After quantitative data collection, 15 respondents were identified who were willing to participate in the qualitative study. Hence, 15 in-depth interviews were conducted at the respondent’s home. Interviews were audio recorded, interviews were lasted for 20-30 minutes.
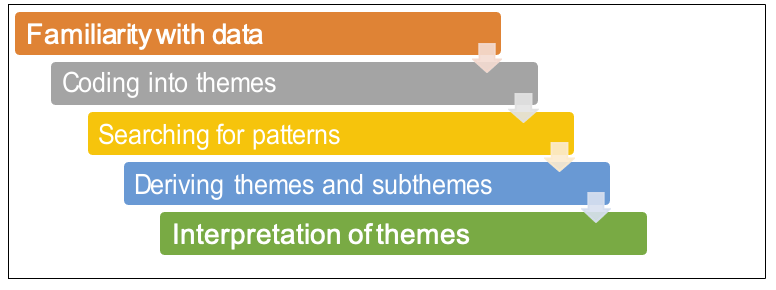
The recorded qualitative interviews were transcribed and translated parallelly to avoid error possibilities and ensure data quality. The transcripts were taken down in the local language and simultaneously transcribed into English. The transcripts were stored on a password-protected computer. Further, the thematic analysis was, inherently a flexible method useful for helpful in identifying key themes. Two independent researchers later coded. Data output from these reports was further synthesized into five meaningful major themes and sub-themes to draw connections between recurrent patterns and themes.


Ethical considerations
The study conducted was part of a master’s dissertation. Therefore, student institutional ethical clearance was obtained from the Savitribai Phule Pune University. The written consent form was provided to the participants to read by themselves and after the approval and confirmation. All the personal information concerning their consent is guaranteed to be confidential as per ethical considerations.
RESULTS
Quantitative results
Table 1 shows the socio-demographic characteristics of selected respondents. The mean age of respondents was 25 years. About 4% of the women underwent early pregnancy i.e., below 18 years of age. The mean age of educational years reported by the extensive respondents was ten years (SD 3.48). About 81.9% of women completed their secondary education, 4.2% completed their primary education, whereas only 11.9% completed their upper secondary education. The highest population was of the Hindu religion, with about 91.5% and only 8.5% belonged to the religion Muslim. Categorizing further, most respondents belonged to the Scheduled Caste (SC) category at 38.1%, followed by the Open Category at 28.8% and the Other Backward Category (OBC) at 15.8%. The least 9.6% formed the Scheduled Tribe (ST) category. More than half 52.7% formed the joint family category whereas 47.3% counted the nuclear family category. had two children whereas 8.5%
Table 2 describes the type of disrespect and abuse experienced by respondents. Non-consented (not being asked for consent from the mother or her accompanying family members before conducting any medical procedures) was highly reported with 35.8%, followed by non-confidential care (patient’s privacy not maintained) with 32.7%. Physical abuse (the delivering mother being beaten up by the health care staff such as nurses, cleaning staff, and also doctors) experienced by the delivering women accounted for up to 16.5%, non-dignified care ( the patients and their accompanying family members being verbally abused or made to clean the bed, etc. after the delivery) with 13.1%, and abandonment of care (absence of clean, proper beds and other necessary facilities) with 11.9%.
Qualitative Results
In support of the quantitative results showing that mistreatment and disrespect among delivering mothers are prevalent, the qualitative result adds to it. The qualitative analysis strongly elaborates on the personal experiences of abusive treatment faced by the individual delivering mothers.
Emerging themes and sub-themes
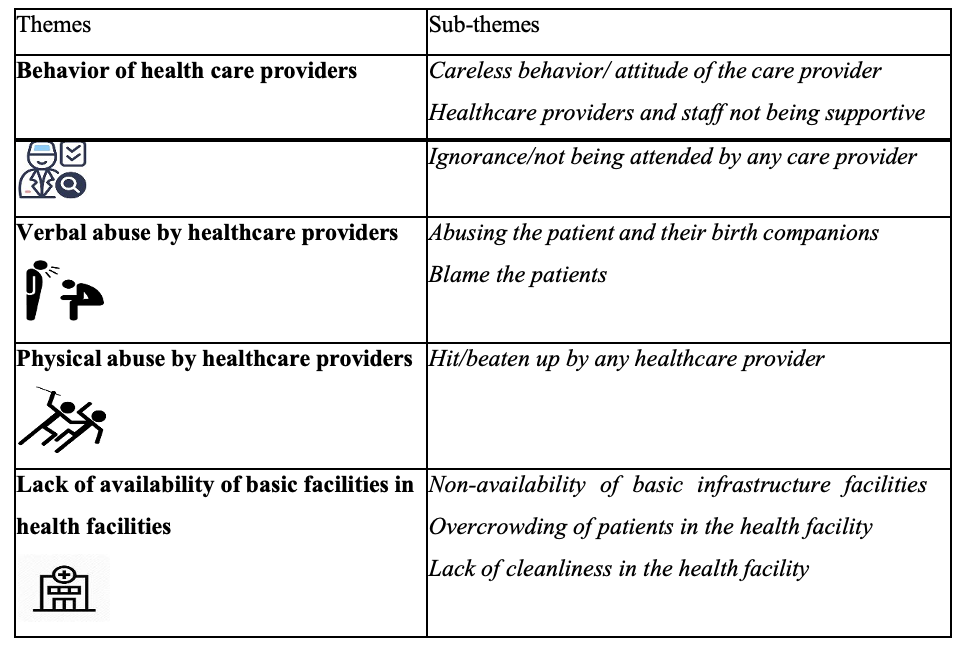
Theme I: Behavior of health care providers
This theme has been further categorized into three sub-themes elaborating on the kind of behavior or attitude the healthcare providers reported by many women during interviews.
Sub-theme 1: Careless behavior/ attitude of care provider
The sub-theme emphasizes a healthcare provider’s careless behavior/attitude, such as ignoring the patient while they were in need, making women wait for longer than needed before taking them to the labor room and delaying treatment.
-
'I was feeling terrible pain but still, they waited until my respective doctor came examined, and treated me
-
‘Care providers were ill-treating me they were putting their hands inside & just kept checking’. I was going through, but they didn’t take me to the labor room and just kept checking.
Sub-theme 2: Healthcare providers and staff not being supportive
The lack of support from health care providers and the staff was one of the prevalent practices that affected the care-seeking by women. It has been reported that providers do not supply the necessary support a woman needs while delivering a baby - when she may be separated from her family. There was also mention of how the healthcare providers deny the patient’s
family members from entering the labor room. Some respondents also reported that healthcare providers pass derogatory comments and use abusive words.
-
'Those people there troubled me a lot during delivery. Those people kept me waiting and didn’t even care to look after me even once. Another cleaning staff was continuously taunting me and saying nothing to me.
-
'Didn’t allow relatives/family, even mother to enter. They shooed away my family every time they came.
Sub-theme 3: Ignorance/not being attended by any care provider
Many of the women recalled being kept waiting and not being attended to for a long time - sometimes overnight. Another respond other respondent described a similar incident where she was kept waiting overnight in pain without being attended to by anyone.
-
'kept me waiting overnight. Nevertheless, those people didn’t even bother to treat me and avoided me.
-
'When we took her (my sister) to the hospital, firstly they only didn’t pay attention to her. In public facilities, as I know, the doctors and specialist nurses, don’t pay much attention.
Theme II: Verbal abuse by the healthcare providers
This theme involves the incidences when delivering women were abused or threatened. The healthcare providers shouted at them while conducting the delivery. The patients and family members accompanying the patient were also being abused or threatened sometimes.
Sub-theme 1: Abusing the patient and their birth companions
The majority of the women mentioned that the medical staff, especially the nurses, always kept shouting and abusing the patients. Especially the hospitalized delivered women who were Shouted at t hem if their babies happened to cry at night. Housekeeping and cleaning staff in the hospital were also involved in the abuse, they shouted at the women and their relatives. Apart from them, the doctors also shouted at patients asking them to keep calm, which could be explained politely. Sometimes, patients were also mistreated on the grounds of the language barrier. Respondents accompanying family members were disrespected and abused by the healthcare providers at delivery time. The healthcare providers were ill-treating them and also were asked to clean the delivery beds.
-
The woman reported, ’ Not the doctors, but the nurses constantly kept yelling and shouting at everyone’. Already going through lots of pain, the ladies who came for cleaning also kept shouting at me.
-
'They just keep getting angry and hyper. At night, when babies usually cry that time, these nurses keep yelling. Doctors and others also abused a lady due to the language barrier.
-
‘Nurse that was there kept scolding my mother all the time’.
-
‘Nurse and cleaning staff that was there kept scolding my mother all the time to keep cleanliness’.
Sub-theme 2: Blame the patients
This theme focuses on how the healthcare providers blamed women for being pregnant again after already having several children. They ill-treated her and kept saying offensive things to her the entire delivery process without respecting her personal choices.
- 'Doctor shouted and blamed me a lot. They forcefully asked me to agree to the operation as I already had three girls. They started talking about anything which I felt was offensive, like they said You already had 3 girls Now again, you are pregnant.
Theme III: Physical abuse to the patient
Sub-theme 1: Hit/beaten up by any healthcare provider
Physical abuse by healthcare providers was a major problem observed in public facilities. It has been reported that adolescent-delivering mothers are especially being harassed. One such incidence had been reported in our study where the girl was just 18 years old at the time of her delivery. She witnessed a terrible experience and was shouting, because of which she was being harassed physically and beaten up on her thighs by the doctors and nurses while delivering. The girl was hit by the instruments such as the blade, which counts as the utmost physical abuse. A similar incident was reported by the other woman in the study as she was beaten up and the healthcare provider forcefully pulled her legs. Also, one woman reported that the nurses who were present at the time of delivery hit her despite the presence of a doctor. Nonetheless, many women from the study reported the same incidences of being brutalized by the doctors/nurses because the patients shouted at the time of delivery due to extreme labor pain.
-
‘Nurses and staff used to hit with sticks. Nurse hit a girl on her thighs as she was making noise’.
-
‘Doctors who came to conduct delivery were beating me. Kept beating me and also hurt me with the blade’.
-
‘constantly beating me. They were pulling my legs so forcefully’.
Theme IV: Lack of availability of basic facilities
The mentioned theme focuses on the availability of basic infrastructure facilities and cleanliness in health facilities. Additionally, overcrowding in public facilities contributes to an overload of patients, leading to a lack of available resources in the healthcare facility.
Sub-theme 1: Non-availability of basic infrastructure facilities
Insufficient beds are available in the public facilities, with mattresses laid on the floor as an alternative, indicating the lack of basic facilities available in the hospitals. One of the experiences shared by a respondent was that women were made to vacate the bed immediately after her delivery, resulting in broken stitches.
'Unavailability of sufficient beds so some patients were kept on c-section beds while some on the mattresses lay on the floor. No bedcovers are available.
'I was made to get down the bed immediately as there were no beds for other patients, because of which my stitches were broken.
Sub-theme 2: Overcrowding of patients in the health facility
Overcrowding in public facilities has been causing a burden on the available essential resources such as medicine, etc., leading to a shortage of medicines or essential resources when needed. Sometimes, respondents’ family members were asked to get medicines from outside due to shortages caused due to overburdening.
‘Hospitals loaded with patients’
Sub-theme 3: No cleanliness in the health facility
Many of the respondents reported that there was no cleanliness maintained in the public
facilities. Most participants reported that the bed covers are never cleaned, and the hospitals are in very unhygienic conditions, which increases the risk of catching other infections.
- 'There is no cleanliness at all
DISCUSSION
The present study revealed that nearly about 40% of women experienced various forms of abusive treatment and disrespect during childbirth in health facilities. One-third of respondents reported non-consented care, and 32% reported non-confidential care. Our study results are consistent with recently published studies in India and worldwide.9,11 The study also reported that 11.9% of women experienced the abandonment of care and 16.5% experienced physical abuse. This is an extreme violation of women’s human rights and puts women at an elevated risk of postpartum complications. The study respondents belonged to the poor socio-economic status thus, experienced higher levels of mistreatment. Previously conducted studies also Supported the same evidence proving that women from poor socio-economic strata, backward religions, and castes experienced significantly higher obstetric violence.11,14
Qualitative results also further confirm that the experience of abusive treatment during childbirth in health facilities is a reality, and women who experienced disrespect were emotionally offended. It demonstrated the harassment of human rights physically as well as verbally, poor health infrastructure, lack of cleanliness, overcrowding, and lack of beds and other resources further stress the women in need.
Abusive treatment during childbirth may have profound consequences on the child’s future health and the mother’s future health. A key implication of our findings is that efforts to increase facility-based delivery must address issues of disrespect and abuse to ensure higher utilization by women and safeguard women’s fundamental rights during facility delivery. The inclusion of conservation of human rights and the patients’ dignity should be included in the medical education curriculum, which can be effective in reducing the issue in the long run.18 Focusing on maternal and child health can effectively prove to lower the incidences of mistreatment and abuse. Strict laws should also be enforced which can optimally reduce the occurrences of the incidences. This study, therefore, offers insight into better health of child and mother by focusing on the elimination of disrespectful incidences during childbirth.19–22
Study limitations
Though the study results highlighted important issues, the study also has certain limitations to note here. The study was conducted in slum communities in urban India, which has distinctive characteristics; therefore, study results may not generalized to other settings. Further, the study adopted a mixed method approach, first collecting quantitative information about the mistreatment and disrespect during facility births in the health care setting, then selecting 15 respondents to proceed with qualitative data collection. Therefore, underreporting or overreporting may not be ruled out completely. Further, recall bias in reporting the exact act of mistreatment and disrespect possible. We also note that disrespect and mistreatment reported in the quantitative study are to get an overall idea of the practice but not to provide any estimations.
CONCLUSIONS
Despite limitations, the study findings are crucial in understanding the prevailing nature of mistreatment and disrespect in health facilities during childbirth in urban areas. The study’s findings suggest that 40% of recently delivered women had experienced disrespect and mistreatment, such as physical and verbal abuse, abandonment of care, and non-consented and non-confidential care. The study indicates that women who delivered in public facilities were more likely to experience any form of disrespect and abuse than in private facilities.
Ethical considerations
The study conducted was part of a master’s dissertation therefore student institutional ethical clearance was obtained from the Savitribai Phule Pune University. The written consent form was provided to the participants to read by themselves and after the approval and confirmation. All the personal information concerning their consent is guaranteed to be confidential as per ethical considerations.
Acknowledgment
We thank all the participants of the study for their valuable contributions. Gratefully acknowledge support from all the organizations involved and contribute to the study’s conduction. The authors are the only contributors to this manuscript and are acknowledged.
Funding
The author(s) received no financial support from any institution for the conducted research, authorship, and/or publication of the article.
Declaration of conflict of interest
The author(s) declare no potential conflict of interest concerning the research, authorship, and/or publication of the article.
Correspondence to:
Miss. Saddichha Marathe
Savitribai Phule Pune University Address: Aundh, Pune, India 411007, India.
email: saddichham@gmail.com